This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
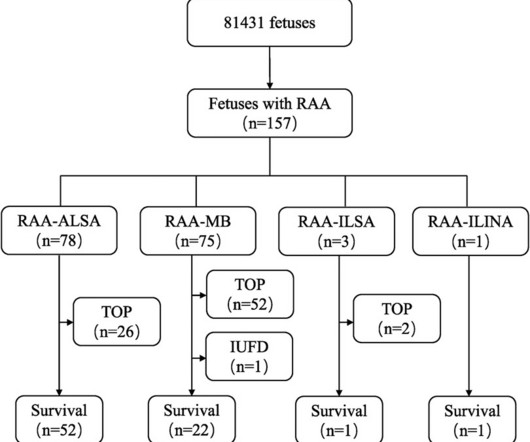
RAA features were characterised by comparing prenatal ultrasound data with anatomical casting results after pregnancy termination or postnatal imaging and surgical intervention to analyse the prognosis and misdiagnoses of fetal RAA.ResultsOf the 157 fetal RAA cases, 50 (31.8%) cases were isolated RAA and 107 (68.2%) cases were nonisolated RAA.
This is the first ever video podcast on EM Cases with Jordan Chenkin from EMU Conference 2017 discussing how to optimize three aspects of cardiac arrest care: persistent ventricular fibrillation, optimizing pulse checks and PEA arrest, with code team videos contrasting the ACLS approach to an optimized approach.
The algorithm uses deep learning to analyse routine ultrasound scans of the heart ( echocardiograms ) to detect disease that often goes undetected during standard assessments. For more information: [link] References: 1 Maurer M, Elliott P, Comenzo R, et al. Circulation. 135(14):1357-1377. 2 Siddiqi O., Trends Cardiovasc Med.
Pioneering techniques have emerged since the previous consensus in 2017, 3 requiring new advice on who should receive this procedure and how to perform it in the safest and most effective manner,” Tzeis added. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation.
Methods We analyzed a cohort of patients admitted for ACS between February 2017 and February 2018. A pulmonary ultrasound was performed on admission and was considered positive (PE+) when there were three or more B-lines in two quadrants or more of each hemithorax. The sensitivity of an NT-proBNP value more than 3647 was 88.9% (51.9–99.7%),
Carotid ultrasound results were divided into two groups based on the presence or absence of plaque. Lp(a) levels were categorized into two groups: below 50 mg/dl and 50 mg/dl or higher. Coronary artery calcium score CT results were analyzed in two groups: CACS=0 and CACS>0.Results:A Results:A total of 2620 subjects were enrolled.
A majority (62.5%) of those presenting with ‘normal’ ECGs had the cath lab activated without any ECG being labeled ‘STEMI’ by automated interpretation – based on signs of Occlusion MI including ECG changes, regional wall motion abnormality on bedside ultrasound, or refractory ischemia. 2017 ; 24 ( 1 ): 120 - 124 2. Acad Emerg Med.
In this study — Procainamide was superior to Amiodarone for terminating monomorphic VT, as well as having fewer adverse effects than Amiodarone ( Ortiz et al — Eur Heart J 1;38 (17): 1329-1335, 2017 ). Procainamide, like Quinidine is a Type 1A antiarrhythmic. Administration of Procainamide is 10-17 mg/kg at 20 mg/min.
You use an ultrasound. 2017 Aug 21;38(32):2459-2472. 2017 Aug 21;38(32):2459-2472. Regardless of the murmur findings they describe. Because using the sounds of a murmur you hear with a stethoscope that was invented in the 1700s is NOT how you make a diagnosis today. Which can now be used easily at the bedside. Eur Heart J.
Beware a negative Bedside ultrasound. I’ve excerpted in Figure-1 , relevant paragraphs from a 2017 ESC ( European Society of Cardiology ) article on this subject by Xanthopoulos & Skoularigis ( ESC: Vol. 15-9/6/2017 ). Pericarditis? Figure-1: Excerpt from ESC review on acute pericarditis ( See text ).
A bedside cardiac ultrasound was performed with a parasternal long axis view demonstrated below: There is a large pericardial effusion with collapse of the right ventricle during systole. 2017 Nov;35(4):525-537. The beat-to-beat variation in QRS amplitude and morphology is electrical alternans. This patient is only pseudo-stable.
My bedside ultrasound was of insufficient quality, but showed somewhat reduced overall EF, distended IVC without respiratory variation, no pericardial effusion, and diffuse bilateral B lines. == What do you think of her ECG? The diagnosis is not easy (see below).
Jeffery Dormu was a double board certified vascular surgeon who was paid $13 million dollars by Medicare alone between 2013 and 2017. A lower extremity arterial ultrasound revealed elevated velocities in the right proximal superficial femoral artery. These payments made him one of the highest paid vascular surgeons in the country.
Many of these issues were described in a prior post by Dr. Angie Lobo ( @aloboMD ) (For open-access reviews of this literature, see Saw 2016 , Saw 2017 , or Hayes 2018.) Often, intravascular ultrasound or intravascular optical coherence tomography is requeried to make the diagnosis.
So I immediately left the room to get an ultrasound machine. While calling for some help and arranging to have her transported to our critical care zone, I got this quick ultrasound which confirmed my suspicion: This quick view was all I was able to obtain in the circumstances. Prac 15(17), 2017.
To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. Here are a couple shots with strain, or "speckle tracking" on ED Echo: hyperacute T-waves speckle 1 x4 from Stephen Smith on Vimeo. hyperacute T-waves speckle 2 x4 from Stephen Smith on Vimeo.
J Electrocardiology 50(5):561-569; September/October 2017. This was missed by the physicians, even with a bedside speckle tracking ultrasound: no wall motion abnormality was seen. Go here to find excel applets. you enter the [link] The closer the formula value is to the cutpoint of 18.2, the more accurate.
Check : [vitals, SOB, Chest Pain, Ultrasound] If the patient has Abdominal Pain, Chest Pain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Good History and Physical exam, including a. Sivilotti, M.,
This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). A bedside cardiac ultrasound revealed grossly normal to hyperdynamic systolic function with no obvious areas of wall motion abnormalities. This was recorded about 30 minutes later: Same A previous ECG was obtained and was normal.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content