This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Clinically: Initial treatment of AFlutter is the same, regardless of whether the rotation direction is CW or CCW — so this distinction is not important to the emergency provider ( Cosio — Arrhythmia & EP Review 6(2):55-62, 2017 ). And a Final Tracing. Reviews PEARLS regarding the ECG diagnosis of AFlutter — and — What's "New"?
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
Abstract Introduction The utility of ablation index (AI) to guide ventricular tachycardia (VT) ablation in patients with structural heart disease is unknown. Methods Consecutive patients ( n = 103) undergoing initial VT ablation at a single center from 2017 to 2022 were evaluated.
While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. Additionally, the qR morphology, particularly in a patient with right bundle branch block (RBBB) type wide QRS complex tachycardia (WQCT), lends further support for VT. What is the rhythm?
In all probability, this dilation is a form of atrial tachycardia and atrial cardiomyopathy. Spatial relationship of sites for atrial fibrillation drivers and atrial tachycardia in patients with both arrhythmias July 2017 International Journal of Cardiology 248(3) AF begets AF. Implications for electrophysiologists.
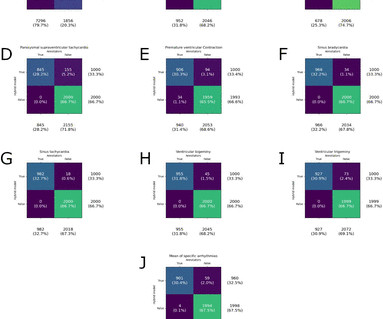
Performance was best for pause (F 1 Score, 99%) and worst for paroxysmal supraventricular tachycardia (F 1 Score, 92%). for paroxysmal supraventricular tachycardia. We calculated classifier statistics for each arrhythmia, all arrhythmias and strips where the model identified normal sinus rhythm. for pause to 7.2%
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
Background:In diabetic ketoacidosis (DKA), cardiac complications such as QTc interval prolongation can pose a risk for ventricular tachycardia. Circulation, Volume 150, Issue Suppl_1 , Page A4143624-A4143624, November 12, 2024. Inclusion criteria encompassed patients under 21 years with two 12-lead ECGs taken during and after DKA resolution.
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. I suspected no OMI, that this could be due to LVH plus tachycardia. Conclusion: Type II MI probable due to hypoxia and tachycardia from resp arrest and amphetamine use. On arrival to the ED, the patient was diaphoretic, tachycardic.
But there are 3 other wide beats in the tachycardia that begins with beat #6 ( = beats #7; 13,14 ). Most Torsades is the result of a pause-dependent effect that predisposes to development of the malignant arrhythmia ( Dohadwala et al — Heart Rhythm Case Rep 3(2):115-119, 2017 ).
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
POTS stands for postural orthostatic tachycardia syndrome. Let’s call it Postural Orthostatic Tachycardia Syndrome – that’s not really a diagnosis – it’s just a medical jargon filled term for what the patient has just told us. What is POTS? When you examine them, the heart rate can be found to be excessively fast.
I’ve excerpted in Figure-1 , relevant paragraphs from a 2017 ESC ( European Society of Cardiology ) article on this subject by Xanthopoulos & Skoularigis ( ESC: Vol. 15-9/6/2017 ). Before discussing my thoughts on interpretation of ECG in this case — it may be helpful to review some of the ECG criteria f or acute pericarditis.
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
Prac 15(17), 2017. One looks for sinus tachycardia and diffuse low voltage but many conditions produce these nonspecific findings. For an excellent review of the pathophysiological explanation of signs and symptoms associated with Pericardial Tamponade SEE this Review by Jensen et al in the e-Journal Card.
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This patient was having recurrent episodes of polymorphic ventricular tachycardia with an underlying long QT interval ( = Torsades des Pointes ). ECG #2 Interpretation of ECG #2: Underlying sinus rhythm.
Introduction:Supraventricular tachycardia (SVT) is known to affect children and teenagers predominantly but can also occur in adults. to -3.33]), followed by a gradual decline till 2017 (7.8) (APC -0.66 [95% CI -2.04 to 2017 (0.6) (APC -2.71), followed by a rise back to 1.0(2020) in adults (above 25 years) from 1999 to 2020.
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. He required multiple defibrillations within a period of a few hours.
ACS QID 75345 In 2017, the New England Journal of Medicine published the results of the Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation (RE-DUAL PCI) trial. His exam was notable for tachycardia, elevated jugular venous pressure, diffuse rales, and an early 2/6 systolic murmur loudest at the cardiac apex.
So now there was ACS + electrical instability, another indication for emergent angiogram. The initial troponin was 5300 ng/L (normal < 17), which corresponded to the symptoms and confirmed subacute occlusion. Shroff, G. & Smith, S. Posterior reperfusion T-waves: Wellens' syndrome of the posterior wall.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Heart Rhythm, 15(9): 1394-1401. [7]
2017 Mar;110(3):188-195. Type 2/3 ECG which gets converted to type 1 pattern with sodium channel blockers have 2 points. J Cardiovasc Electrophysiol. 2020 Sep;31(9):2474-2483. Gourraud JB, Barc J, Thollet A, Le Marec H, Probst V. Brugada syndrome: Diagnosis, risk stratification and management. Arch Cardiovasc Dis.
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Heart 2002;87:220228 This 2017 article by Vandenberk B et al. I (Smith) measure the QT at 320 ms The Bazett-corrected QTc is divided by square root of 0.36 which is 0.6 So is it really prolonged?
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Most physicians will automatically be worried about these symptoms. Thiruganasambandamoorthy, V., Sivilotti, M., Mukarram, M., Baumann, B.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
PEARL #4: Electrical alternans is most commonly encountered by emergency providers in association with supraventricular tachycardias ( especially for the reentry SVT rhythms of AVRT and AVNRT ). Although other entities may produce various forms of alternans ( as discussed in the Oct.
There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. Here is a similar case: Collapse, Ventricular Tachycardia, Cardioverted, Comatose on Arrival. Agitation, Confusion, and Unusual Wide Complex Tachycardia. There is sinus tachycardia at ~115/minute.
CMAJ 2017 Vassallo SU, Delaney KA, Hoffman RS, et al. The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy. Indian Pacing Electrophysiol J 2004 Antzelevitch C, Yan G. J wave syndromes. Heart Rhythm 2010 Hudzik B, Gasior M. J-waves in hypothermia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content