This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
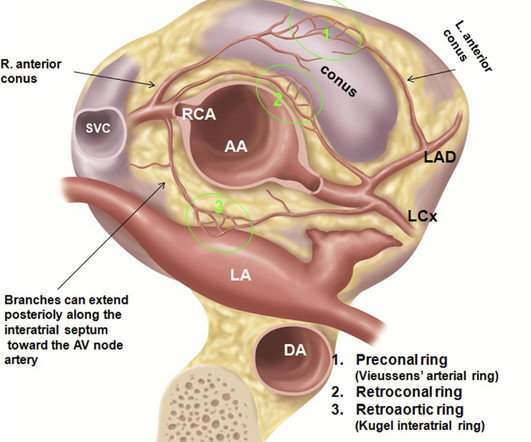
Agarwal ,et al Radiographics 2017 ) Left main Atresia: Is it a sub-set of the anomalous origin of LCA from the right sinus ? Final message Coronary arterial anomaly is a less discussed topic nowadays, unless & until, it intrudes an interventional cardiologist in his daily routine life, of delivering stents. Annu Rev Physiol.
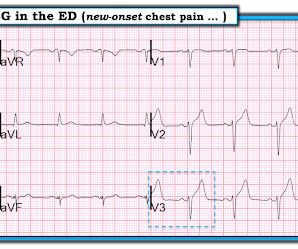
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. He was found to have a 100% circumflex lesion for which a bare metal stent was placed.
Computer interpretation: SINUS RHYTHM NON-DIAGNOSTIC ANTEROLATERAL ST ELEVATION BORDERLINE ECG The overreading cardiologist confirmed the computer interpretation (did not diagnose OMI or STEMI). Since the threshold for "STEMI" is 2.0 mm, this ECG actually meets STEMI criteria. Since the threshold for "STEMI" is 2.0
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. He was rushed to the Cath Lab where an LAD culprit lesion was stented. Here is the LAD after stent placement. As the conversation progressed, another ECG spontaneously printed. The pathology is now painfully evident.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. A mid-LAD culprit lesion was identified and stented. Smith comment : V5 and V6 are excessively discordant!!!! & Desai, M. Josephson, M.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc J Electrocardiology 50(5):561-569; September/October 2017. Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Case 4 Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04
There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI). Troponin I returned 80 ng/mL, and the Cath Lab was then reactivated where a 100% LAD occlusion was found and stented.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. It was stented. She called 911. Learning Points : 1. See this case.
distal stent patent. PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. This figure comes from the Diamond T study (all type 1 MI were NSTEMI, not STEMI): Notice that the 6 hour value (far right) is very low for type 2 MI.
This doesn’t meet STEMI criteria so in the current paradigm there’s no urgency to getting an angiogram. The initial ECG suggested either subacute or reperfused inferoposterior occlusion and clearly does not meet traditional STEMI criteria. Discharge diagnosis was ‘STEMI’, even though no ECG ever met STEMI criteria.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content