This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Different ST-segment elevation myocardial infarction (STEMI) localizations go along with dissimilarities in the size of the affected myocardium, the causing coronary vessel occlusion, and the right ventricular participation. Results Of the 2,195 patients, 1,118 had an anterior (AWS)- and 1,077 a non-anterior-wall-STEMI (NAWS).
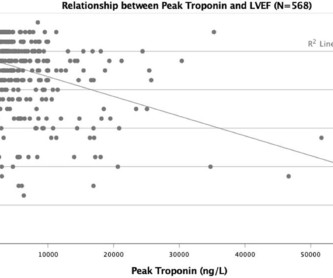
Background The clinical significance of peak troponin levels following ST-elevation myocardial infarction (STEMI) has not been definitively established. Methods A single-centre retrospective observational study was conducted of all patients with STEMI between January 2015 and December 2017. The mean age was 63.6±12
Acad Emerg Med 2017; 24(1): 120 – 24. The cath lab was activated, as it should be with transient STEMI. See this case of transient STEMI: Spontaneous Reperfusion and Re-occlusion - My Bad Thinking Contributes to a Death. It is not yet available, but this is your way to get on the list. link] Hughes KE et al. Learning Points 1.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). 2017 Sep-Oct;50(5):561-569. Epub 2017 Apr 19. There is high QRS voltage.
EGE was collected at 3 minutes after contrast agent injection, where hyperintense areas (signal intensities > mean+2SD of remote myocardium) were considered as the area at risk, plus the hypointense core within.
Methods:STEMI patients who underwent coronary revascularization therapy and cardiac magnetic resonance (CMR) at about 4 days and 6 months between 2017 and 2023 were included. The patients were divided into groups (Group 1, FSF (-) during procedures with final TIMI-3; Group 2, FSF (+) with TIMI-3; Group 3, final angiogram was non-TIMI-3).
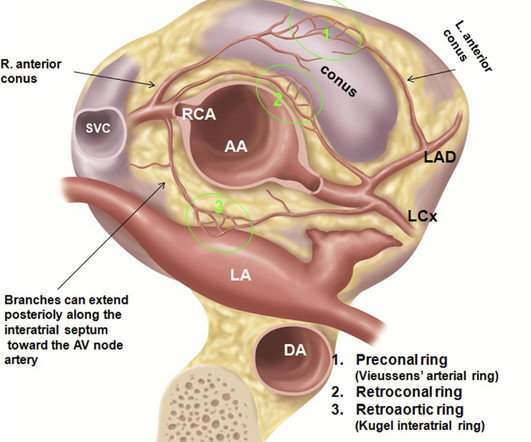
Agarwal ,et al Radiographics 2017 ) Left main Atresia: Is it a sub-set of the anomalous origin of LCA from the right sinus ? We know, how adverse is the outcome of Left main STEMI. Right arising from the left sinus is much more commoner than left arising from the right. This topic of anomalous origin needs a separate discussion.
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. January 2017. There is also ST elevation in lateral precordial leads V5 and V6.
Had the cardiologists followed NSTEMI or transient STEMI guidelines, which recommend non-urgent cath, the patient could have redeveloped an OMI and had a worse outcome. But this foresight will not be recorded, because the patient was diagnosed as "transient STEMI", even though no ECG ever met STEMI criteria.
Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). 21, 2017 ). Post PCI the patient became gravely hypotensive and "shocky". She stabilized on dobutamine and levosimendan infusions that could be discontinued after 24 hours. The LV EF was 57% at formal echo.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. So maybe she is better than I am.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. In this study — Procainamide was superior to Amiodarone for terminating monomorphic VT, as well as having fewer adverse effects than Amiodarone ( Ortiz et al — Eur Heart J 1;38 (17): 1329-1335, 2017 ). The below ECG was recorded.
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
Computer interpretation: SINUS RHYTHM NON-DIAGNOSTIC ANTEROLATERAL ST ELEVATION BORDERLINE ECG The overreading cardiologist confirmed the computer interpretation (did not diagnose OMI or STEMI). Since the threshold for "STEMI" is 2.0 mm, this ECG actually meets STEMI criteria. Since the threshold for "STEMI" is 2.0
As per Dr. Aslanger — a number of medical providers were initial confused by what initially appears as marked ST elevation with reciprocal ST depression, indicative of an acute STEMI. That was also my initial concern. No "baseline" ECG is available for comparison.
ACS QID 75345 In 2017, the New England Journal of Medicine published the results of the Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation (RE-DUAL PCI) trial. Explanation: The EKG illustrates an inferior STEMI. Click here for a free trial. Sample Cardiology Board Review Practice Questions Question 1.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. Smith comment : V5 and V6 are excessively discordant!!!! Here are two examples of HATW’s in the setting of confirmed LVH. & Desai, M.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc J Electrocardiology 50(5):561-569; September/October 2017. Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Case 4 Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04
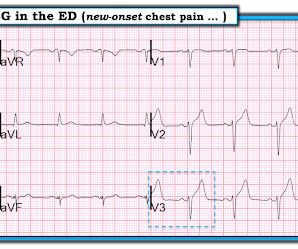
European Heart Journal 38(41):3082-3089; November 1, 2017. And, in cases like the elderly patient with new-onset chest pain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. BOTTOM LINE: Despite cardiac pacing — ECG #2 is diagnostic of a very large acute anterior STEMI.
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center. As the conversation progressed, another ECG spontaneously printed. 2] Driver, B.
Angie Lobo ( @aloboMD ) (For open-access reviews of this literature, see Saw 2016 , Saw 2017 , or Hayes 2018.) A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. A study by Hassan et al. Lobo et al. where more than 3/4 of cases were NSTEMI).
There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI). 1] Vitals BP 160/110 HR 90 (trend) RR 24 (BBS CTA) SaO2 92% RA Attached is the Patient's ECG. link] [1] Zachary et al.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. Patients with transient occlusion may manifest only transient STEMI on ECG.
PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. This figure comes from the Diamond T study (all type 1 MI were NSTEMI, not STEMI): Notice that the 6 hour value (far right) is very low for type 2 MI. Angiogram: LM 30% ostial.
JACC 69(23):1694-1703; April 4, 2017. But lead V2 has a worrisome amount of ST elevation, and in a chest pain patient, I would be worried about STEMI. S-wave is in V2 = 17 mm S-wave V4 = 9 mm Total = 26 (not greater than 28), so not LVH by the new rule! Nevertheless, it has the look of LVH. Peguero JG et al.
normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? I’ve excerpted in Figure-1 , relevant paragraphs from a 2017 ESC ( European Society of Cardiology ) article on this subject by Xanthopoulos & Skoularigis ( ESC: Vol. 15-9/6/2017 ).
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
This paper by Bischof and Smith compared inferior MI to pericarditis and found that of 154 patients with inferior STEMI, 17% of whom had less than 1 mm of STE in any inferior lead, all 154 had at least 0.25 Prac 15(17), 2017. mm STE depression in aVL.
This doesn’t meet STEMI criteria so in the current paradigm there’s no urgency to getting an angiogram. The initial ECG suggested either subacute or reperfused inferoposterior occlusion and clearly does not meet traditional STEMI criteria. Discharge diagnosis was ‘STEMI’, even though no ECG ever met STEMI criteria.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). Further history later: This patient personally has no further high risk features (syncope / presyncope), but her mother had sudden cardiac arrest in sleep. Syncope and ST Segment Elevation. And another finding.
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! West J Emerg Med 2017. HyperKalemia with Cardiac Arrest. References 1. Lindner et al. Eur J Emerg Med 2020. Durfey et al. Farkas et al.
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). This correlates with potentially salvageable myocardium. See Raitt et al.: These findings together are more commonly seen with pericarditis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content