This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Different ST-segment elevation myocardialinfarction (STEMI) localizations go along with dissimilarities in the size of the affected myocardium, the causing coronary vessel occlusion, and the right ventricular participation. No significant associations of the STEMI localization with long-term mortality were found.
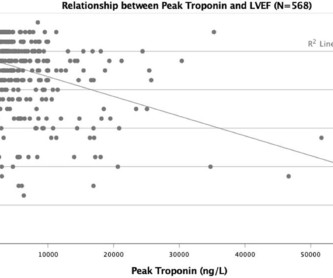
Background The clinical significance of peak troponin levels following ST-elevation myocardialinfarction (STEMI) has not been definitively established. Methods A single-centre retrospective observational study was conducted of all patients with STEMI between January 2015 and December 2017. The mean age was 63.6±12
Acad Emerg Med 2017; 24(1): 120 – 24. The cath lab was activated, as it should be with transient STEMI. See this case of transient STEMI: Spontaneous Reperfusion and Re-occlusion - My Bad Thinking Contributes to a Death. It is not yet available, but this is your way to get on the list. link] Hughes KE et al.
BACKGROUND:T2-weighted imaging is commonly used to measure myocardial salvage in reperfused myocardialinfarction but is hindered by poor reproducibility and indistinct boundaries. The median MSI was 35.0% (interquartile range, 22.959.5%), with smaller MSI observed in patients with larger infarcts (P<0.001).
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). 2017 Sep-Oct;50(5):561-569. Epub 2017 Apr 19. There is high QRS voltage.
Methods:STEMI patients who underwent coronary revascularization therapy and cardiac magnetic resonance (CMR) at about 4 days and 6 months between 2017 and 2023 were included. The patients were divided into groups (Group 1, FSF (-) during procedures with final TIMI-3; Group 2, FSF (+) with TIMI-3; Group 3, final angiogram was non-TIMI-3).
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. January 2017. There is also ST elevation in lateral precordial leads V5 and V6.
LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid. PCI mid LCx So this is an OMI (Occlusion MyocardialInfarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk.
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
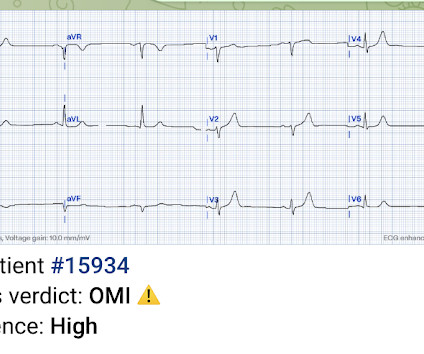
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). The below ECG was recorded. Inotropic medication was continued.
Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. Impact of total occlusion of culprit artery in acute non-ST elevation myocardialinfarction: a systematic review and meta-analys is.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department.
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center. As the conversation progressed, another ECG spontaneously printed. 2] Driver, B.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc J Electrocardiology 50(5):561-569; September/October 2017. Annals of Emergency Medicine 2012;60:45-56.
Angie Lobo ( @aloboMD ) (For open-access reviews of this literature, see Saw 2016 , Saw 2017 , or Hayes 2018.) A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. A study by Hassan et al. Lobo et al. where more than 3/4 of cases were NSTEMI).
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
Smith: T waves are very hyperacute: these are a sign of ACUTE infarction, even if there are Q-waves. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). See Raitt et al.:
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content