This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This update summarizes relevant clinical data published since the 2017 American Heart Association scientific statement on KD related to diagnosis, cardiac imaging in acute KD treatment, and long-term management. Recent data have advanced the understanding of safety and dosing for several anti-inflammatory therapies in KD.
or basilar ischemia. 2017 Sep-Oct;50(5):561-569. Epub 2017 Apr 19. Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization. EKG on arrival to the ED is shown below: What do you think? However, T waves do not appear to be hyperacute or hyperkalemic. J Electrocardiol.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This is the initial ECG: The QRS is widened with a regular cadence, and there are no discernable P waves.
In the STEMI/NSTEMI dichotomy, NSTEMI is supposed to mean non-occlusive myocardialinfarction, but this patient had transient Occlusion MI that was at risk for re-occlusion (like ‘transient STEMI’). Impact of total occluson of culprit artery in acute non-ST elevation myocardialinfarction: a systemic review and meta-analysis.
Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardialinfarction. It’s important to stress the presence of a normal QRS (i.e., References 1] Smith, S. Annals of Emergency Medicine, 60 (1), 45-56. 2] Driver, B.
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. There is also a Q-wave in III. There is also subtle STD in V3-V5. The initial troponin I was elevated at 0.75
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. J Electrocardiology 50(5):561-569; September/October 2017. This makes it almost certain that the ST elevation on the first one is due to ischemia. Annals of Emergency Medicine 2012;60:45-56.
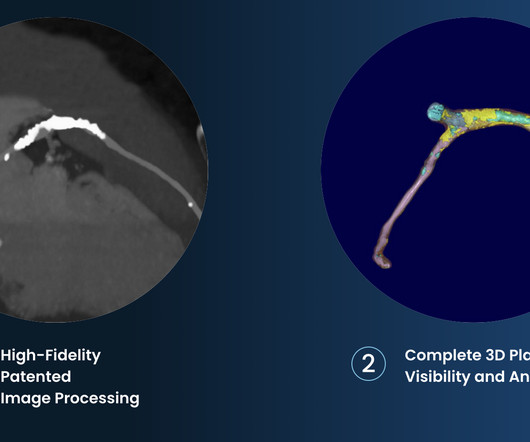
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. The 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS).”
Cardiovascular disease is the most common cause of death and disability globally, largely driven by myocardialinfarction and ischemic stroke caused by atherosclerosis (plaque build-up in the arteries). 2017 23, April 2020; Available from: [link]. Cardiovasc. 6 (3) (2019).
LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid. PCI mid LCx So this is an OMI (Occlusion MyocardialInfarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk.
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 Efficacy and Safety of Low-Dose Colchicine after MyocardialInfarction. 4 In the U.S. 12 Colchicine, 0.5 34 Colchicine, 0.5 N Engl J Med.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Comparison of the QRS complex, ST-segment, and T-wave among patients with left bundle branch block with and without acute myocardialinfarction.
Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. Impact of total occlusion of culprit artery in acute non-ST elevation myocardialinfarction: a systematic review and meta-analys is.
In most cases, rather, the culprit is gross ischemia due to myocardialinfarction, cardiomyopathy, or advanced coronary artery disease. Unfortunately, today’s case is lacking any such diagnostics, thus I cannot say with certainty that the QT interval is, or is not, culpable in arrhythmogenesis. [1] 2] Viskin, S., 3] Murphy, M.
Evidence of acute ischemia (may be subtle) vii. to 1.64) for myocardialinfarction or death from coronary heart disease, and 1.06 (95 percent confidence interval, 0.77 Old myocardialinfarction, 6. ST segment and T wave abnormalities consistent with or possibly related to myocardialischemia.
It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis. Due to the atypical and vague symptoms, the myocardialinfarct was not initially diagnosed. At presentation he had a history of dyspnea for 6 days.
Clinical questions : Is this an occlusion myocardialinfarction and does the patient need the cath lab? CMAJ 2017 Vassallo SU, Delaney KA, Hoffman RS, et al. Occurrence of “J Waves” in 12-Lead ECG as a Marker of Acute Ischemia and Their Cellular Basis. Heart Rhythm 2010 Hudzik B, Gasior M. J-waves in hypothermia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content