This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Safety of Computer Interpretation of Normal Triage Electrocardiograms. Acad Emerg Med 2017; 24(1): 120 – 24. The cath lab was activated, as it should be with transient STEMI. See this case of transient STEMI: Spontaneous Reperfusion and Re-occlusion - My Bad Thinking Contributes to a Death. link] Hughes KE et al.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI." He was worried for inferior MI and ordered another, which was recorded 15 minutes later: Now clearly and obviously diagnostic of inferior STEMI. January 2017. There is also ST elevation in lateral precordial leads V5 and V6. References : 1.
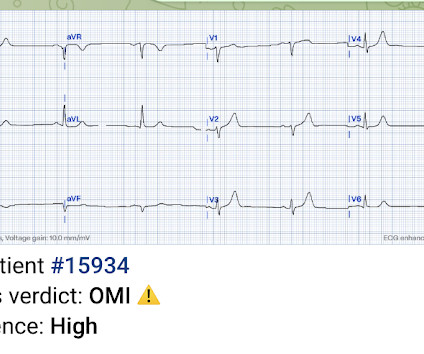
An initial electrocardiogram (ECG) is provided below. As per Dr. Aslanger — a number of medical providers were initial confused by what initially appears as marked ST elevation with reciprocal ST depression, indicative of an acute STEMI. The patient was promptly admitted to the hospital for further evaluation. What do you think?
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. So maybe she is better than I am. Heart Rhythm, 13(7): 1515-1520. [2]:
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardial infarction in the emergency department.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Bicarb 20, Lactate 4.2,
PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. This figure comes from the Diamond T study (all type 1 MI were NSTEMI, not STEMI): Notice that the 6 hour value (far right) is very low for type 2 MI. Angiogram: LM 30% ostial.
A Deep Neural Network learning algorithm outperforms a conventional algorithm for emergency department electrocardiogram interpretation. JACC 69(23):1694-1703; April 4, 2017. But lead V2 has a worrisome amount of ST elevation, and in a chest pain patient, I would be worried about STEMI. What an honor. Peguero JG et al.
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). Fever not only unmasks a Brugada-type electrocardiogram (ECG) but also increases the risk of ventricular tachyarrhythmias such as ventricular fibrillation (VF) or sudden cardiac death. Syncope and ST Segment Elevation.
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! Severe hyperkalemia: can the electrocardiogram risk stratify for short-term adverse events. West J Emerg Med 2017. HyperKalemia with Cardiac Arrest. References 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content