This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. He did not remember whether he had experienced any chestpain. (TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Two subsequent troponins were down trending.
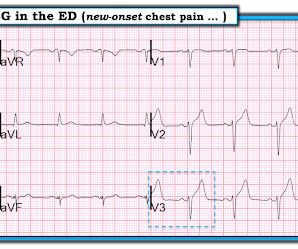
male was sitting at a work conference when he began having substernal chestpain with diaphoresis. The pain was 7 out of 10 when this ECG was recorded: The QTc = 375 What do you think? Here is the post stent ECG: This is probably the amount of ST elevation (zero) that this patient has at baseline.
TheNational Institute for Health and Care Excellence(NICE) recommends CCTA as the first-line investigation for patients with chestpain due to suspected CAD, highlighting its importance in improving diagnostic certainty. Curr Cardiovasc Imaging Rep (2017) 10: 15. Available at: [link]. AccessedFebruary 2023 vii Moss AJ et al.
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina. All is fixed.
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. link] Here is the history: A 30 yo man presented complaining of severe chestpain.
J Electrocardiology 50(5):561-569; September/October 2017. This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
Factors consistently manifesting as such, in addition to chestpain, include, diaphoresis, vomiting, radiation of pain (most alarming when inclusive of both arms), and pain aggravated by exertion. [1] Troponin I returned 80 ng/mL, and the Cath Lab was then reactivated where a 100% LAD occlusion was found and stented.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. A mid-LAD culprit lesion was identified and stented. Below are two examples of this. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution.
It was stented. 12 Example Cases of Use of 3- and 4-variable formulas, plus Simplified Formula, to differentiate normal STE from subtle LAD occlusion 3. . == == MY Comment by K EN G RAUER, MD ( 10/23/2020 ): == There are a number of important lessons worthy of repeating from today's repost of our case from March 28, 2017.
Delayed angiogram found a 95% mid RCA occlusion that was stented. Eur Heart J 2017 Driver BE, Shroff GR, Smith SW. Smith : this proves my impression that the inferior T-waves on the first ECG are hyperacute. Notice also that there is new T-wave inversion in III with upright T-wave in aVL, confirming inferior infarction.
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the Emergency Department with sudden onset chestpain that began 14-hours ago. The pain improved (6/10) but is persisting, which prompted him to visit the Emergency Department. What do you think?
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content