This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren Four patients presented with chestpain. 4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6]
male was sitting at a work conference when he began having substernal chestpain with diaphoresis. The pain was 7 out of 10 when this ECG was recorded: The QTc = 375 What do you think? Since the threshold for "STEMI" is 2.0 mm, this ECG actually meets STEMI criteria. Since the threshold for "STEMI" is 2.0
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." examined SCAD presenting as STEMI (unlike Hassan et al.
A 61 year-old with chestpain arrived to the ED by ambulance with resolving chestpain. Acad Emerg Med 2017; 24(1): 120 – 24. The chestpain is resolving, so if these are resolving hyperacute T-waves, then followup ECGs should show their size diminishing. This ECG is NOT normal. Learning Points 1.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). 2017 Sep-Oct;50(5):561-569. Epub 2017 Apr 19. There is high QRS voltage.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death.
A 65 year old with diabetes presented with a syncopal episode while sitting, associated with weakness but no chestpain or shortness of breath. Had the cardiologists followed NSTEMI or transient STEMI guidelines, which recommend non-urgent cath, the patient could have redeveloped an OMI and had a worse outcome.
Just the fact of chestpain and highly elevated troponin is enough to activate the cath lab, but here you can see just how subtle hyperacute T-waves can be. Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). 21, 2017 ). Post PCI the patient became gravely hypotensive and "shocky".
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. This is diagnostic of inferior MI, though does not meet millimeter criteria for "STEMI."
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc J Electrocardiology 50(5):561-569; September/October 2017. Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Case 4 Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04
Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. There is some ST-segment elevation in DII, DIII, aVF, V4-6. Due to the observed ST-segment elevation, the medical team expressed immediate concern.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion.
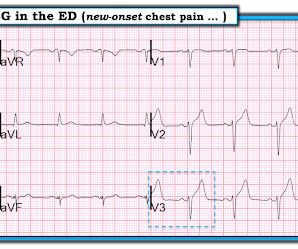
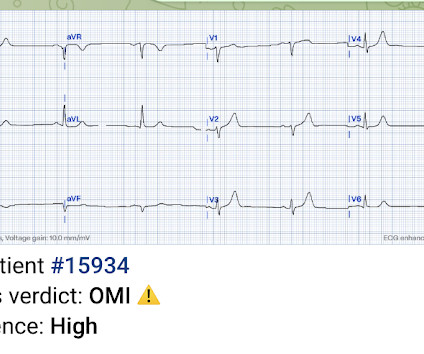
Case An elderly patient had acute chestpain and 911 was called. European Heart Journal 38(41):3082-3089; November 1, 2017. And, in cases like the elderly patient with new-onset chestpain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. What do you think?
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
ACS QID 75345 In 2017, the New England Journal of Medicine published the results of the Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation (RE-DUAL PCI) trial. Explanation: The EKG illustrates an inferior STEMI. Click here for a free trial. Sample Cardiology Board Review Practice Questions Question 1.
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e.
JACC 69(23):1694-1703; April 4, 2017. But lead V2 has a worrisome amount of ST elevation, and in a chestpain patient, I would be worried about STEMI. All bets would be off if instead of no chestpain, this patient had worrisome new-onset symptoms. Nevertheless, it has the look of LVH. Peguero JG et al.
Factors consistently manifesting as such, in addition to chestpain, include, diaphoresis, vomiting, radiation of pain (most alarming when inclusive of both arms), and pain aggravated by exertion. [1] It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS).
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. It was from a patient with chestpain: Note the obvious Brugada pattern. Bicarb 20, Lactate 4.2,
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. Also, persistence of a pain free state does not guarantee an open artery.
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. Patient 1 Patient 2 STEMI criteria is based only ST elevation millimeter criteria measured in isolation from the QRS and stratified by age/sex, so this is the only information provided above.
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the Emergency Department with sudden onset chestpain that began 14-hours ago. This doesn’t meet STEMI criteria so in the current paradigm there’s no urgency to getting an angiogram. Shroff, G.
This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. Follow up the next AM: Brugada pattern is resolved Below is what the electrophysiologist recommended. And another finding.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). He presented to the emergency department for evaluation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content