This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Patients who experience acute myocardialinfarction (AMI) are at risk of recurrent AMI. Contemporary data on recurrent AMI and its association with return emergency department (ED) visits for chestpain are needed. Return ED visits for chestpain occurred in 27.0% (2017/7467) of index AMI survivors.
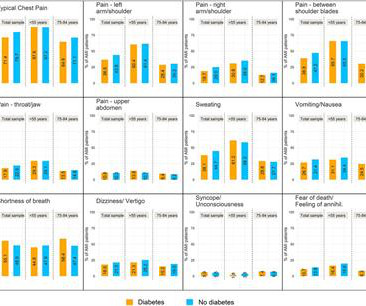
Background The objective of this study was to investigate the differences in presenting symptoms between patients with and without diabetes being diagnosed with an acute myocardialinfarction (AMI). Results Patients with diabetes had significantly less frequent typical pain symptoms, including typical chestpain.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. For more information: www.heartflow.com References 1 Krievins, Dainis K.,
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." References Lobo AS et al. JACC 2019 Sep 10;74(10):1290-1300.
A 61 year-old with chestpain arrived to the ED by ambulance with resolving chestpain. Acad Emerg Med 2017; 24(1): 120 – 24. The chestpain is resolving, so if these are resolving hyperacute T-waves, then followup ECGs should show their size diminishing. This ECG is NOT normal.
Background To determine if the European Society of Cardiology 0/1-hour (ESC 0/1-h) algorithm with high-sensitivity cardiac troponin T (hs-cTnT) meets the ≥99% negative predictive value (NPV) safety threshold for 30-day cardiac death or myocardialinfarction (MI) in older, middle-aged and young subgroups.
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
2017 Sep-Oct;50(5):561-569. Epub 2017 Apr 19. Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization. Not a STEMI: Reasons I did not think ECG #1 represented an acute STEMI — included the following: There was no history of chestpain. J Electrocardiol.
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. link] Here is the history: A 30 yo man presented complaining of severe chestpain.
Case An elderly patient had acute chestpain and 911 was called. Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. European Heart Journal 38(41):3082-3089; November 1, 2017.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. J Electrocardiology 50(5):561-569; September/October 2017. This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
Detailed Considerations LBBB and MyocardialInfarction In the emergent setting it’s important to assess LBBB through the lens of the Smith-modified Sgarbossa criteria, especially in a context that is clinically consistent with Acute Coronary Syndrome. He received a permanent pacemaker during the subsequent inpatient stay. 4] Dodd, K.
In the STEMI/NSTEMI dichotomy, NSTEMI is supposed to mean non-occlusive myocardialinfarction, but this patient had transient Occlusion MI that was at risk for re-occlusion (like ‘transient STEMI’). Impact of total occluson of culprit artery in acute non-ST elevation myocardialinfarction: a systemic review and meta-analysis.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Below are two examples of this.
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. J Electrocardiol 2017 2. Hyperacute T waves can be a useful sign of occlusion myocardialinfarction if appropriately defined. McLaren, Meyers, Smith and Chartier. Acad Emerg Med 2023 3.
Background Long-term prognosis associated with low–high-sensitivity cardiac troponin T (hs-cTnT) concentrations in patients with chestpain is unknown. Patients with myocardial injury (any hs-cTnT >14 ng/L), including patients with myocardialinfarction (MI) were excluded. fold (HR 1.61, 95% CI 1.53
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Old myocardialinfarction, 6. Thiruganasambandamoorthy, V., Sivilotti, M., Mukarram, M.,
Scenario 1 : The patient presents with 24 hours of substernal chestpain. It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis. Most common cause) 2 ) Post infarct regional pericarditis. What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content