This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
He did not remember whether he had experienced any chestpain. This is a critically important determination because of the 2017 AHA/ACC/HRS Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. Within a few days, the patient was extubated and was neurologically intact.
Written by Jesse McLaren Four patients presented with chestpain. 2017 ; 24 ( 1 ): 120 - 124 2. All initial ECGs were labeled ‘normal’ or ‘otherwise normal’ by the computer interpretation, and below are the ECGs with the final cardiology interpretation. Hughes KE , Lewis SM , Katz L , Jones J. Acad Emerg Med.
Contemporary data on recurrent AMI and its association with return emergency department (ED) visits for chestpain are needed. Methods This Swedish retrospective cohort study linked patient-level data from six participating hospitals to four national registers to construct the Stockholm Area ChestPain Cohort (SACPC).
male was sitting at a work conference when he began having substernal chestpain with diaphoresis. The pain was 7 out of 10 when this ECG was recorded: The QTc = 375 What do you think? This was recorded at the Controversies and Consensus Lecture I gave in Northampton MA in September 2017.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." A similar episode had occurred a week earlier during labor.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. Journal of Vascular Surgery, Mar. 2024, [link]. 301–302, [link]. 22, 30 Nov.
TheNational Institute for Health and Care Excellence(NICE) recommends CCTA as the first-line investigation for patients with chestpain due to suspected CAD, highlighting its importance in improving diagnostic certainty. Curr Cardiovasc Imaging Rep (2017) 10: 15. Available at: [link]. AccessedFebruary 2023 vii Moss AJ et al.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death.
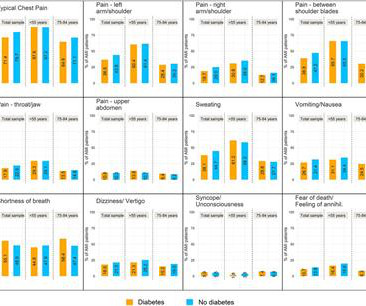
All patients aged between 25 and 84 years were recorded by the population-based Myocardial Infarction Registry in Augsburg, Germany, between 2010 and 2017. Results Patients with diabetes had significantly less frequent typical pain symptoms, including typical chestpain.
A 61 year-old with chestpain arrived to the ED by ambulance with resolving chestpain. Acad Emerg Med 2017; 24(1): 120 – 24. The chestpain is resolving, so if these are resolving hyperacute T-waves, then followup ECGs should show their size diminishing. This ECG is NOT normal.
Methods We conducted a subgroup analysis of adult emergency department patients with chestpain prospectively enrolled from eight US sites (January 2017 to September 2018).
A 65 year old with diabetes presented with a syncopal episode while sitting, associated with weakness but no chestpain or shortness of breath. PEARL #1: Not all patients with acute MI report chestpain. Not all patients with acute ( or recent ) MI have chestpain. What do you think?
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
Just the fact of chestpain and highly elevated troponin is enough to activate the cath lab, but here you can see just how subtle hyperacute T-waves can be. 2) Typical persistent chestpain with a sigificantly elevated troponin is OMI until proven otherwise, regardless of the ECG. 21, 2017 ).
2017 Sep-Oct;50(5):561-569. Epub 2017 Apr 19. Not a STEMI: Reasons I did not think ECG #1 represented an acute STEMI — included the following: There was no history of chestpain. J Electrocardiol. doi: 10.1016/j.jelectrocard.2017.04.005. 2017.04.005. PMID: 28460689. Lee DH, Walsh B, Smith SW.
Abstract Aims ‘Hot phases’, characterized by chestpain and troponin release, may represent the first clinical presentation of arrhythmogenic cardiomyopathies. In patients with apoptosis at EMB, left ventricular ejection fraction was lower at first clinical presentation and improved during follow-up with anti-neurohormonal therapy.
J Electrocardiology 50(5):561-569; September/October 2017. This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5
This was sent by : Jacob Smith, DO Emergency Medicine Resident Ohio Health Doctors Hospital Emergency Residency Christopher Lloyd, DO, FACEP Director of Clinical Education, USACS Midwest Case A 30 year old patient presents to triage with chestpain. link] Here is the history: A 30 yo man presented complaining of severe chestpain.
Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. There is some ST-segment elevation in DII, DIII, aVF, V4-6. Due to the observed ST-segment elevation, the medical team expressed immediate concern.
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
ACS QID 75345 In 2017, the New England Journal of Medicine published the results of the Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation (RE-DUAL PCI) trial. Click here for a free trial. Sample Cardiology Board Review Practice Questions Question 1. Question 2.
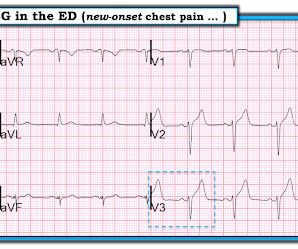
Case An elderly patient had acute chestpain and 911 was called. European Heart Journal 38(41):3082-3089; November 1, 2017. And, in cases like the elderly patient with new-onset chestpain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. What do you think?
Whether stenting a narrowed coronary artery improves symptoms such as chestpain (angina) or shortness of breath is a very different question. However, the devil is in the detail when considering this question, and I have discussed it in more detail here. What About Symptoms?
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
JACC 69(23):1694-1703; April 4, 2017. But lead V2 has a worrisome amount of ST elevation, and in a chestpain patient, I would be worried about STEMI. All bets would be off if instead of no chestpain, this patient had worrisome new-onset symptoms. Nevertheless, it has the look of LVH. Peguero JG et al.
Factors consistently manifesting as such, in addition to chestpain, include, diaphoresis, vomiting, radiation of pain (most alarming when inclusive of both arms), and pain aggravated by exertion. [1] It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS).
Diagnosis : Atrial flutter with 1:1 conduction, with fast AV conduction made possible by sympathetic drive of exercise On arrival, we obtained another 12-lead: Unremarkable Further history: One month history of shortness of breath on exertion, denies palpitations, chestpain, orthopnea, leg swelling.
It was from a patient with chestpain: Note the obvious Brugada pattern. For now, the 2017 AHA/ACC/HRS guidelines for asymptomatic patients that have inducible types of Brugada syndrome recommend observation without any specific therapies or interventions [8]. There is no further workup at this time.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. Below are two examples of this. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution. & & Desai, M. Manual of Cardiovascular Medicine (5th ed.).
Smith and Myers found that in otherwise classic Wellens syndrome – that is, prior anginal chestpain that resolves with subsequent dynamic T wave inversions on the ECG – even the T waves of LBBB behave similarly. [2] 2] Although the clinical context in today’s case does not fit these descriptors for Type I OMI (e.g. 2] Meyers, H.
. == == MY Comment by K EN G RAUER, MD ( 10/23/2020 ): == There are a number of important lessons worthy of repeating from today's repost of our case from March 28, 2017. Serial ECGs correlated to the presence ( and severity ) of chestpain — often reveal the status of the "culprit" artery (ie, occluded, reopened, reoccluded ).
There was no chestpain — and all troponins were negative. Walsh & Smith in our January 4, 2017 post — in which there are Q waves suggesting a pseudo - infarction pattern. Smith immediately knew he needed to find out what was going on with this patient! It turned out the patient had cardiac amyloidosis.
She denied chestpain and denied feeling any palpitations, even during her triage ECG: What do you think? Her symptoms started suddenly about 48 hours ago, but had continued to worsen, including epigastric discomfort, nausea, cough, and dyspnea and lightheadedness on exertion. The diagnosis is not easy (see below).
Eur Heart J 2017 Driver BE, Shroff GR, Smith SW. Smith : this proves my impression that the inferior T-waves on the first ECG are hyperacute. Arch Cardiovasc Dis 2013 Khan AR et al. Impact of total occluson of culprit artery in acute non-ST elevation myocardial infarction: a systemic review and meta-analysis. Emerg Med J 2017;34(2):119–23.
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the Emergency Department with sudden onset chestpain that began 14-hours ago. The pain improved (6/10) but is persisting, which prompted him to visit the Emergency Department. What do you think?
the optimum QT correction formula for patients with chestpain was found to be unique for each individual ; it is a correction factor that can be calculated real-time for each patient by taking multiple measurements over a range of heart rates. --Malik M et al. Heart 2002;87:220228 This 2017 article by Vandenberk B et al.
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. J Electrocardiol 2017 2. Patient 1 (ECG on the left) was a 45 year-old male, and patient 2 (ECG is on the right) was a 70 year-old male. McLaren, Meyers, Smith and Chartier.
They are always tired, they have bad brain fog, they have issues with lack of refreshing sleep, they have horrendous gut issues, they have chestpain and breathlessness, they have headaches and they even have bladder symptoms. What do they mean when they say they feel rubbish all the time?
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? 2017 Nov;35(4):525-537. She was noted to be tachycardic and her heart sounds were distant on physical exam. She had a normal respiratory effort, and her lungs were clear to auscultation bilaterally. 2013.06.023.
Background Long-term prognosis associated with low–high-sensitivity cardiac troponin T (hs-cTnT) concentrations in patients with chestpain is unknown. Conclusion Patients with chestpain and undetectable hs-cTnT have an overall lower risk of death compared with the general population, with risks being highly age dependent.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Thiruganasambandamoorthy, V.,
This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. Follow up the next AM: Brugada pattern is resolved Below is what the electrophysiologist recommended.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. Ninety percent of patients with reperfusion attained a maximum T wave negativity of 3 mm or more within 48 hours after the onset of chestpain in the lead that initially displayed the greatest ST segment elevation. Below is his presentation ECG.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content