This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
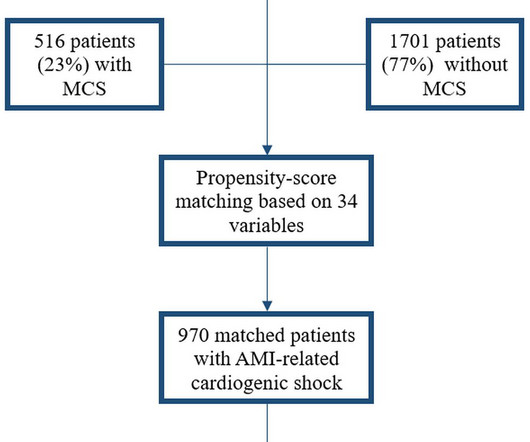
Background Despite limited beneficial evidence, mechanical circulatory support (MCS) is commonly used in patients with acute myocardialinfarction-related cardiogenicshock (AMI-CS). In this Dutch registry, we investigated MCS usage, associated patient characteristics and clinical outcomes.
The patient in today’s case presented in cardiogenicshock from proximal LAD occlusion, in conjunction with a subtotally stenosed LMCA. Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ).
Admissions to CICUs with the highest tertile of CCRx utilization had a greater burden of comorbidities, had more diagnoses of ST–elevation myocardialinfarction, cardiac arrest, or cardiogenicshock, and had higher Sequential Organ Failure Assessment scores. CCRx was provided to 62.2% (interhospital range of 21.3%–87.1%)
LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid. PCI mid LCx So this is an OMI (Occlusion MyocardialInfarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. The patient went into cardiogenicshock and ultimately died of this MI. The cath lab was activated.
Many of these issues were described in a prior post by Dr. Angie Lobo ( @aloboMD ) (For open-access reviews of this literature, see Saw 2016 , Saw 2017 , or Hayes 2018.) were pretty sick, with mostly LM/pLAD lesions and high rates of cardiogenicshock. Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The Society (..)
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content