This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
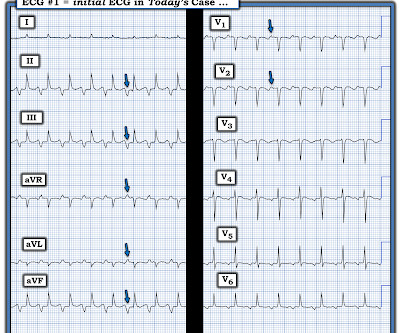
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. 2016, April 13). The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). He was intubated for altered mental status.
I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute. Sinus Tachycardia and RAD — as already noted above. PEARL # 2: In the absence of associated heart failure ( cardiogenic shock ) — sinus tachycardia is not a common finding in acute MI.
It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenic shock). As per Dr. Frick — sinus tachycardia is usually not seen with acute OMI unless the patient is in cardiogenic shock. Both were wrong.
Founded by three physicians and a data scientist in 2016 in Marseille, France, the company’s mission is to improve cardiac arrhythmia management by developing state-of-the-art, data-driven medical devices trained on large databases of procedural data.
TANGO2 deficiency disorder (TDD), identified in 2016, affects more than 8,000 individuals worldwide. One of its defining traits is the susceptibility to QTc prolongation and life-threatening ventricular tachycardia (VT) that resists most conventional treatments, significantly reducing patients’ life expectancy.
You are shown the ECG in Figure-1 — told only that the patient had a “continuous" tachycardia. PEARL # 4: This less common form of "fast-slow" AVNRT that is illustrated in Figure-3 — has also been known as an "incessant" tachycardia. ECG Blog #138 — AFlutter vs Atrial Tachycardia. What is the differential diagnosis?
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
Among 475 patients with cardiac sarcoidosis, 119 (25.1%) were isolated cardiac sarcoidosis (iCS) based on the 2016 Japanese Circulation Society criteria. iCS was diagnosed according to the 2016 Japanese Circulation Society (JCS) guidelines.
Methods This observational study assessed single-chamber ICD recipients implanted from 2006 to 2016 from Boston Scientific's ALTITUDE database and linked to the NCDR ICD Registry. We sought to determine predictors of RV pacing in patients who did not have a pacing indication at the time of initial ICD implant.
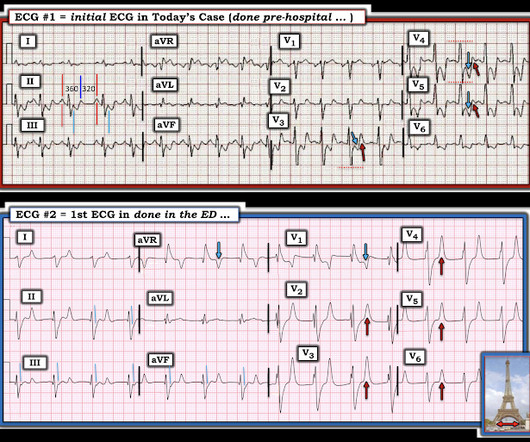
Here is the only prehospital 12-lead: Sinus tachycardia, somewhat wide QRS, Ischemia Here is the first ED ECG: What is the rhythm here? Medics found patient in PEA arrest. He was resuscitated into a perfusing rhythm. He went in and out of arrest until arrival at the ED.
ECG in a person with persistent anginal pain for the past several hours showing significant ST segment depression anterolateral leads along with sinus tachycardia. 2016 Sep;68 Suppl 2(Suppl 2):S226-S227. 2016; 6:49-51. ST segment elevation is noted in aVR. Clinical evaluation and X-Ray chest showed features of pulmonary edema.
His prehospital ECG showed "inferior" ST depression and high voltage, with tachycardia. I suspected no OMI, that this could be due to LVH plus tachycardia. Conclusion: Type II MI probable due to hypoxia and tachycardia from resp arrest and amphetamine use. On arrival to the ED, the patient was diaphoretic, tachycardic.
Other trials that evaluated this subject were the WOEST trial (2013), Pioneer AF-PCI trial (2016), and ISAR-TRIPLE (2015). His exam was notable for tachycardia, elevated jugular venous pressure, diffuse rales, and an early 2/6 systolic murmur loudest at the cardiac apex. These are the main aspects of the findings related to this trial.
Tachycardia (or nearly) 2. Tachycardia, = 1.8. Finally , they found these independent predictors of PE: Note that tachycardia only has an Odds ratio of 1.8. Tachycardia is unusual in ACS unless there is cardiogenic shock or a second simultaneous pathology. Some providers were worried about ACS because of this ECG.
Shanghai Score was arrived at in a consensus conference held in 2016. 2016 Oct;13(10):e295-324. Spontaneous type 1 ECG has the highest number of points at 3.5, while fever-induced type 1 ECG has 3 points. Type 2/3 ECG which gets converted to type 1 pattern with sodium channel blockers have 2 points. Heart Rhythm. J Am Coll Cardiol.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. She was ventilated by bag-valve-mask by EMS on arrival and was quickly intubated with etomidate and succinylcholine. A rectal temperature was obtained which read 107.9
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Optimal QT interval correction formula in sinus tachycardia for identifying cardiovacular and mortality risk: Findings from the Penn Atrial Fibrillation Free study. Heart Rhythm 2016 Feb; 13(2):527-35.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. See my quick review of atrial tachycardia below) The tachycardia spontaneously resolved. BP:143/99, Pulse 109, Temp 37.2 °C
had ventricular tachycardia/ventricular fibrillation and 73.4% The primary outcome was inhospital mortality. Multivariable logistic regression analysis was used to adjust for potential confounders. Among 207 770 patients with IHCA, 26.6% had pulseless electrical activity/asystole.
However, the effects of sacubitril/valsartan on these outcomes, as well as on ventricular tachyarrhythmias, have not been well studied in women with HFrEF.MethodsThis study included consecutive series of patients treated with sacubitril/valsartan at University Hospital Mannheim from 2016 to 2020. vs. 0.6%; p=0.121) (2.3% vs. 10.1%; p=0.762).
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. 2016) in the presence of spontaneous BrS ECG or drug-induced ECG.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Most physicians will automatically be worried about these symptoms. The tracings were considered abnormal in the following cases: 1.
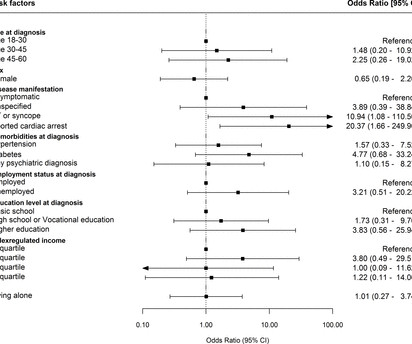
Methods and results In this nationwide cohort study, all patients diagnosed with cLQTS in Denmark between 1996 and 2016 aged 18–60 years at diagnosis were identified using nationwide registries. to 249.9); ventricular tachycardia/syncope OR 10.9 (95% Patients attached to the workforce at diagnosis were included. 95% CI, 1.7
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). This patient very likely has some form of idiopathic ventricular tachycardia. Of the ventricular outflow tract tachycardias (RVOT-VT) makes up 80-90%.
As noted above the presence of acute target organ damage in today's case ( ie, acute MI ) in association with marked sustained hypertension ( this patient's BP at times exceeding 200 mm Hg systolic and >110 mm Hg diastolic ) qualifies her as a true hypertensive emergency ( Janke et al JAHA 5(12); 2016 and Cardiology Advisor Feb.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content