This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
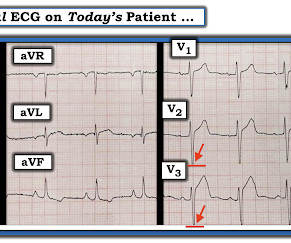
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. But STEMI criteria is only 43% sensitive for OMI.[1]
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Jason was very skeptical of STEMI. This also argues against STEMI. Look for old ECGs Do serial ECGs Do echocardiography June 17, 2016 Anterior STEMI? There was no chestpain.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." examined SCAD presenting as STEMI (unlike Hassan et al.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! But if there is none - then you are looking at least at an Isolated Posterior STEMI until proven otherwise.
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Jason was very skeptical of STEMI. This also argues against STEMI. The diagnostic problem posed in today's repost from June 17, 2016 is a perfect example of this. There was no chestpain.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). 2016 Nov;34(11):2182-2185. Epub 2016 Aug 27. There is high QRS voltage.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. But the History in today's case was acute shortness of breath with dizziness and lightheadedness — and, essentially without chestpain!
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. The patient has a history of CABG so some of these changes could be old, but with ongoing chestpain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. HR 40, BP 135/70, RR16, O2 100%.
He complained of severe chestpain and was extremely agitated, so much so that he was throwing chairs in triage. Technically, the STE meets STEMI criteria because there is greater than 2.5 These kinds of cases were excluded from the study as obvious anterior STEMI. JAMA Internal Med 2016 Dec 1.; What do you think?
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. A patient with OMI can have a totally normal ECG!"
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
It turns out that this was a 27 yo African American male who presented with pressure-like (non-pleuritic) chestpain and dyspnea. Here is a case of a 45 year old with chestpain: There is ST elevation in inferior leads only, with no reciprocal ST depression in aVL. Would you be certain that it is not STEMI?
Other trials that evaluated this subject were the WOEST trial (2013), Pioneer AF-PCI trial (2016), and ISAR-TRIPLE (2015). ACS QID 3103 A 64 year old Caucasian male with a history of extensive tobacco use, hypertension, hyperlipidemia, and obesity presents with acute onset chestpain. Incorrect Answers: A and E. Question 2.
Case An elderly patient had acute chestpain and 911 was called. Methods : The PERFECT study (#NCT02765477) is a retrospective, 16 center, international investigation of ED patients from 1/2008 - 12/2016 with VPR on the ECG and symptoms of acute coronary syndrome (ACS). What do you think? in leads with at least 1 mm STE.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. It was from a patient with chestpain: Note the obvious Brugada pattern. Bicarb 20, Lactate 4.2,
Note: according to the STEMI paradigm these ECGs are easy, but in reality they are difficult. Theres inferior STE which meets STEMI criteria, but this is in the context of tall R waves (18mm) and relatively small T waves, and the STD/TWI in aVL is concordant to the negative QRS. This was false positive STEMI with an ECG mimicking OMI.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. They also recommended a NTG drip, after which she reported complete resolution of pain. She was a walk-in at triage.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. In the world of STEMI, we are incapable of recognizing the first ECG as a false negative.
The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. 2016) in the presence of spontaneous BrS ECG or drug-induced ECG. Heart Rhythm 2016. Types 2 and 3 have been merged into Type 2 and look substantially different. Is this Type 2 Brugada syndrome/ECG pattern?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content