This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
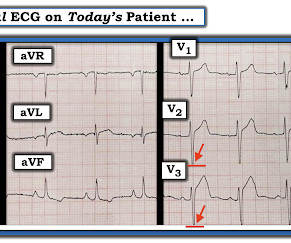
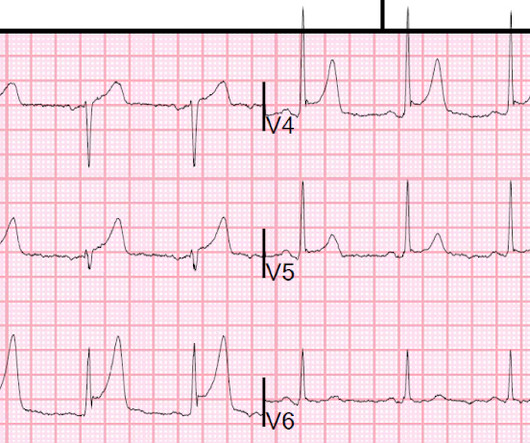
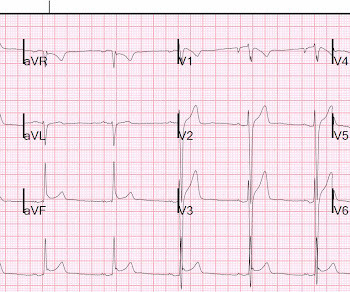
Written by Jesse McLaren, with a very few edits by Smith A 60-year-old presented with chestpain. Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chestpain as a “STEMI equivalent”[3] 3. Am J Emerg Med 2016 5. But are there any other signs of Occlusion MI? Kontos et al. Meyers et al.
Contemporary data on recurrent AMI and its association with return emergency department (ED) visits for chestpain are needed. Methods This Swedish retrospective cohort study linked patient-level data from six participating hospitals to four national registers to construct the Stockholm Area ChestPain Cohort (SACPC).
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Pretest probability: Especially when there is no Chestpain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." A similar episode had occurred a week earlier during labor.
A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. Chestpain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. July 2016. Does routine use of the 15-lead ECG improve the diagnosis of acute myocardial infarction in patients with chestpain? This case comes from Sam Ghali ( @EM_RESUS ). Thanks, Sam! This is his 12-Lead ECG: What do you think?
a med tech company dedicated to helping patients with persistent ischemic heart disease, has announced the treatment of the first patient with the A-FLUX Reducer System, a treatment for patients with angina or chestpain. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation.
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. In this case there had been 100% ventricular pacing since 2016. PLUS — Today's patient is an older woman with known severe coronary disease who presented with new chestpain. What do you think? Our THANKS to Dr.
years]) admitted to the China ChestPain Center Database between 2016 and 2021. Hierarchical clustering of 15 medical conditions was performed to derive multimorbidity patterns. The primary outcome was a composite of inhospital adverse events.
There were no injuries and no chestpain and he appeared well. He complained of 3 days of diarrhea and abdominal pain. Pretest probability: Especially when there is no Chestpain, or there are very atypical symptoms, one should be very suspicious of the diagnosis of coronary occlusion unless the ECG is crystal clear.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
With more than 500 peer-reviewed publications, the HeartFlow FFR CT Analysis remains unparalleled in precision coronary care, as supported by the ACC/AHA ChestPain Guidelines, to improve treatment plans and outcomes. J Nucl Cardiol 2016. 2021 ACC/AHA ChestPain Guidelines. Arbab-Zadeh, Heart Int 2012. NEJM 2010.
A 48 year-old female with hypertension, hyperlipidemia, chronic low back pain, and bilateral lower extremity neuropathy. She presents with chestpain and nonspecific EKG changes undergoes a one day myocardial perfusion stress test with Tc99m Sestamibi. The pass rate for the nuclear cardiology examination in 2016 was 82%.
But the History in today's case was acute shortness of breath with dizziness and lightheadedness — and, essentially without chestpain! Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
2016 Nov;34(11):2182-2185. Epub 2016 Aug 27. Not a STEMI: Reasons I did not think ECG #1 represented an acute STEMI — included the following: There was no history of chestpain. Lee DH, Walsh B, Smith SW. Terminal QRS distortion is present in anterior myocardial infarction but absent in early repolarization. 2016.08.053.
On occasion — such anterior lead ST elevation ( instead of T wave inversion ) can be seen with acute PE ( Zhan et al — Ann Noninvasive Electrocardiol 19(6):543-551, 2014 — and — Omar HR — Eur Heart J: Acute Cardiovascu Care (5(8): 579-586, 2016 ). Right-sided leads such as leads III , aVR and V1 — face the anterior region of the RV.
we analyzed patients presenting from 2016 to 2021 with an initial diagnosis of stroke, defined by ICD-10 codes in any diagnostic position as abstracted from free text responses by ED staff. We therefore used population-level data to report the frequency of cardiac troponin assessments among U.S. 32.2%) had troponin tested in the ED.
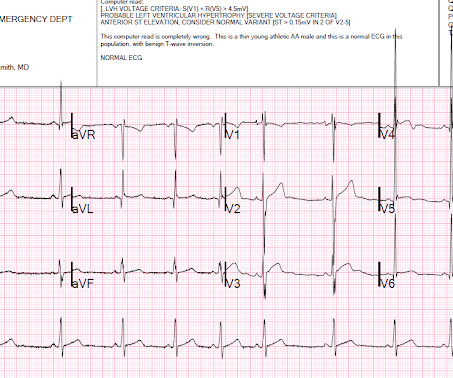
Although the overwhelming majority of young adults presenting for emergency care who manifest ER patterns on ECG have a benign prognosis — there is a small-but-present percentage of such individuals who go on to develop a lethal cardiac arrhythmic event ( Zakka & Refaat- ACC, 2016 ).
And some similar ECGs from Pulmonary Embolism: A young woman with altered mental status and hypotension An elderly woman transferred to you for chestpain, shortness of breath, and positive troponin - does she need the cath lab now?
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
Diagnosis : Atrial flutter with 1:1 conduction, with fast AV conduction made possible by sympathetic drive of exercise On arrival, we obtained another 12-lead: Unremarkable Further history: One month history of shortness of breath on exertion, denies palpitations, chestpain, orthopnea, leg swelling.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. The patient has a history of CABG so some of these changes could be old, but with ongoing chestpain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. Int J Cardiol 2016 3.
He complained of severe chestpain and was extremely agitated, so much so that he was throwing chairs in triage. JAMA Internal Med 2016 Dec 1.; His chestpain resolved. Resolution of ST elevation with resolution of chestpain makes the diagnosis. Case 1: The outcome of this case is at the far bottom.
See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. You do not need to be better than the Queen of Hearts at EKG to understand that refractory chestpain NEEDS CATH NOW.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
It turns out that this was a 27 yo African American male who presented with pressure-like (non-pleuritic) chestpain and dyspnea. Here is a case of a 45 year old with chestpain: There is ST elevation in inferior leads only, with no reciprocal ST depression in aVL. N Engl J Med 2008;358(19):2016-23.
Other trials that evaluated this subject were the WOEST trial (2013), Pioneer AF-PCI trial (2016), and ISAR-TRIPLE (2015). ACS QID 3103 A 64 year old Caucasian male with a history of extensive tobacco use, hypertension, hyperlipidemia, and obesity presents with acute onset chestpain. Incorrect Answers: A and E. Question 2.
Smith and Myers found that in otherwise classic Wellens syndrome – that is, prior anginal chestpain that resolves with subsequent dynamic T wave inversions on the ECG – even the T waves of LBBB behave similarly. [2] 2] Although the clinical context in today’s case does not fit these descriptors for Type I OMI (e.g. 3] Meyers, H.
She denied chestpain and denied feeling any palpitations, even during her triage ECG: What do you think? Her symptoms started suddenly about 48 hours ago, but had continued to worsen, including epigastric discomfort, nausea, cough, and dyspnea and lightheadedness on exertion. In contrast — a broader passband ( typically from 0.05
Case An elderly patient had acute chestpain and 911 was called. Methods : The PERFECT study (#NCT02765477) is a retrospective, 16 center, international investigation of ED patients from 1/2008 - 12/2016 with VPR on the ECG and symptoms of acute coronary syndrome (ACS). What do you think? Data from ten sites are presented here.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. This was done in the October 31, 2016 case on Dr. Smith’s ECG Blog: For clarity — I’ve reproduced this post-Conversion tracing in Figure-2.
the optimum QT correction formula for patients with chestpain was found to be unique for each individual ; it is a correction factor that can be calculated real-time for each patient by taking multiple measurements over a range of heart rates. Heart Rhythm 2016 Feb; 13(2):527-35. In this study by Hasanien et al. ,
It was from a patient with chestpain: Note the obvious Brugada pattern. The elevated troponin was attributed to either type 2 MI or to non-MI acute myocardial injury. There is no further workup at this time. Smith: Here is a case that was just texted to me today from a former resident. This patient ruled out for MI.
Patient 2 : 55 year old with 5 hours of chestpain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This was missed by the treating physician, but the chestpain resolved with aspirin.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. History Patient complains of a 24-hours of chestpain of sudden onset, sharp in nature. Denies SOB.
The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. 2016) in the presence of spontaneous BrS ECG or drug-induced ECG. Heart Rhythm 2016. Types 2 and 3 have been merged into Type 2 and look substantially different. Is this Type 2 Brugada syndrome/ECG pattern?
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. It has been stuttering, lasting 10 minutes at a time with associated diaphoresis.
days of chestpain that started as substernal and crushing in nature awakening him from sleep and occasionally traveling to right side of neck. The pain was described as constant, worse with deep inspiration and physical activity, sometimes sharp. 2016 Apr 12;67(14):1738-49. He reported 1.5 Circulation. doi: 10.1161/CIR.0000000000001001.
He played a round of golf a week prior and felt an episode of chestpain during the round, which spontaneously resolved. On presentation, he reported no chestpain or shortness of breath. Five days later, the patient was exercising when he developed chestpain at 19:30 which lasted for an hour.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content