This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. What About the Tachycardia? Today's regular SVT rhythm could be an ectopic atrial tachycardia ( ATach ) — or an automatic junctional tachycardia.
The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). The cause of the abnormal baseline deflections seen in Figure-2 is most likely muscle tremor artifact ( See Bouthillet T — ACLS Med Training, Dec, 2015 ). Figure-2: I've labeled the initial ECG.
The study of ventriculoatrial (VA) conduction during an electrophysiological (EP) study is crucial for ablating supraventricular tachycardias (SVT) and WPW, particularly with suspected accessory pathways or AV nodal reentry tachycardia.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. 2015, March 1). The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ).
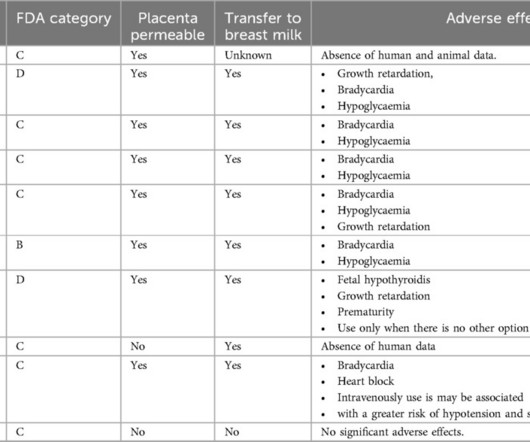
BackgroundPregnancy increases the risk of supraventricular tachycardia (SVT) due to physiological changes. MethodsWe retrospectively analyzed 15 pregnant patients with SVT treated at Shenzhen Second People's Hospital ED from 2015 to 2023. This study reviews the management of SVT in pregnant patients in the emergency department (ED).MethodsWe
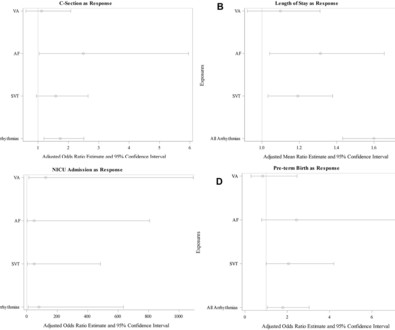
Methods This was a case–control study of women admitted in labour to one of eight hospitals of Northwell Health from January 2015 to June 2021. Objectives Examine the association between arrhythmias and adverse maternal outcomes in women with structurally normal hearts. Arrhythmia was previously diagnosed in 58.0% AF and 8.1%
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
Patients with SP or AVB, 21 years of age or younger, who underwent CNA between 2015 and 2021 were included. with one documented SP after termination of atrial tachycardia at the 3-month follow-up. Objective Describe the methodology and role of CNA for treatment of pediatric patients with functional AVB or SP. The median age was 18.9
T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. NOTE #3: For review of the "many faces" of benign ST-T wave variants — numerous examples are shown and discussed in the March 22, 2022 post by Dr. Meyers — and earlier, in the January 7, 2015 post in Dr. Smith's Blog. What is it? Anterior STEMI?
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
2015 Oct; 66(4):355-362. Hypotension may of course be a result of a brady- or tachydysrhythmia. 2) Hypoxia, including poisons of oxidative phosphorylation such as HS, CO, CN. 3) Anemia, or poisons of hemoglobin such as methemoglobin or CO 4) Fixed coronary stenosis that limits flow. Annals of Emergency Medicine. De Backer D et al.
Chagas disease (ChD) was associated with increased rates of ventricular tachycardia and ventricular fibrillation in ICD patients only in the initial two periods, but there was no statistical difference in the last period. Analysis revealed that period 3 (2015–2018) was associated with better death-free survival ( p = .007).
Other trials that evaluated this subject were the WOEST trial (2013), Pioneer AF-PCI trial (2016), and ISAR-TRIPLE (2015). His exam was notable for tachycardia, elevated jugular venous pressure, diffuse rales, and an early 2/6 systolic murmur loudest at the cardiac apex. These are the main aspects of the findings related to this trial.
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Optimal QT interval correction formula in sinus tachycardia for identifying cardiovacular and mortality risk: Findings from the Penn Atrial Fibrillation Free study. Acad Emerg Med 2015 Oct; 22(10):1139-44.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. She arrived to the ED with a nonrebreather mask. Her blood pressure on arrival was 153/69.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Annals of Emergency Medicine March 2015 ; Volume 65, Issue 3, Pages 268–276.e6 18) Venkatesh Thiruganasambandamoorthy et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content