This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
IntroductionThe 2015 American Heart Association Guidelines recommended mechanical thrombectomy with stent‐retriever devices. Compared with 2012‐2014, the 2015‐2019 cohort showed increased odds of ICH and shock while the odds of DVT, pulmonary embolism, pneumonia, and UTI were significantly lower.
Literature has demonstrated that carotid artery stenting (CAS) poses greater risk of postoperative complications, particularly stroke, than carotid endarterectomy (CEA). Methods The National Inpatient Sample (NIS) was queried for patients undergoing CAS and CEA from 2010 to 2015.
Background:Increased immediate and delayed re-occlusion rates, up to 33%, are reported in patients undergoing acute stenting for tandem lesions, with symptomatic hemorrhage rates around 10-15%. Intraprocedural intravenous (IV) cangrelor is emerging as a bridging therapy for antiplatelet inhibition during acute stenting in ischemic stroke.
Introduction:Current evidence suggests that acute carotid artery stenting (CAS) for cervical lesions is associated with better functional outcomes in patients with acute stroke with tandem lesions (TLs) treated with endovascular treatment (EVT). Stroke, Volume 55, Issue Suppl_1 , Page ATMP94-ATMP94, February 1, 2024.
The American Journal of Emergency Medicine 2015; 33(6):786-790. Former resident: "Just saw cath report, LAD stent was 100% acutely occluded." They of course opened and stented it. Electrocardiographic Criteria to Differentiate Acute Anterior ST Elevation Myocardial Infarction from Left Ventricular Aneurysm. You taught us well!"
We compared clinical and technical outcomes with first‐line stent retriever (SR), contact aspiration (CA), or combined techniques in patients with isolated PCA occlusion.METHODSThis international case–control study was conducted at 30 sites in Europe and North America and included consecutive patients with isolated PCA occlusion presenting within 24 (..)
Previous studies in LVO and MeVO have demonstrated a correlation between good clinical outcomes and the first pass effect (FPE, eTICI 2c/3 on the first pass) but no differences in FPE rates or clinical outcomes between first‐line endovascular therapy techniques.1‐6
The studies were classified in 3 periods by publication date: Period 1: before 2015, pre-stent retriever; Period 2: 2015-2019, early thrombectomy era; and Period 3: 2020-2024, recent period.Results:Of 2693 references, 21 trials met inclusion criteria, 3 in Period 1, 10 in Period 2, 8 in Period 3.
We also compared the safety of acute carotid stenting (CAS) in TLs with low ASPECTS.Methods:This prospective multicenter study from 16 centers included patients with anterior circulation TL from 2015-2020. in patients with stenting (18/44) versus no-stenting (25/44).Conclusion:This 3.05; p=0.32), PH2 (OR: 1.14, CI: 0.26-5.02;
Navigation beyond the occlusion and retraction of stent‐retriever/aspiration catheter were the two most common procedural steps that led to perforation.ConclusionIn our cohort, perforation was approximately twice as frequent in MeVO than in LVO thrombectomy. The primary outcomes were independent functional outcome (i.e.
Intravascular imaging (IVI), such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), play a crucial role in assessing lesion characteristics and optimizing stent placement during percutaneous coronary intervention (PCI). Patients were divided into two groups based on IVI usage.
Just before 10 AM, the patient received a stent to the culprit OM. We know that today's patient has had prior inferior OMI with stenting of his proximal RCA ~3 years earlier. In this view, the culprit lesion is not particularly obvious which is an important principle in angiography, and the reason why we obtain multiple views.
Methods:Our study comprised 1390 adult patients diagnosed with LVO stroke that underwent endovascular therapy at Rhode Island Hospital from July 2015 to March 2023 and data collected retrospectively. In the ICADLVO group, 23 out of 68 patients underwent angioplasty, whereas 38 patients received stenting.
Our primary endpoint was complete/near-complete reperfusion (eTICI 2c-3) at pass #2 (after pass #1 failure). Secondary endpoints included 1) eTICI2b-3 at pass#2, and 2) eTICI2c-3 with pass #3 (following failure in two consecutive passes with the same technique).
Unfortunately, we do not have those images for review, but the operators described a ruptured LAD plaque and they stented this area, which ensures the stability of the plaque. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region.
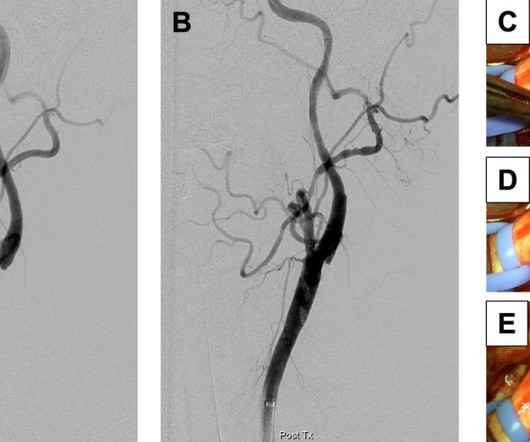
5 ICSS‐ MRI study (International Carotid Stenting Study Magnetic Resonance Imaging Study), indicated that patients with periprocedural hemodynamic depression had decreased cerebral blood flow and increased the risk of new lesions in imaging.6 This is secondary to delayed postoperative cerebral ischemia and infarction caused by vasospasm.7
American Heart Journal 170(6):1255-1264; December 2015. There is no ST depression in lead I, which suggests a circumflex lesion The cath lab was activated and a circumflex occlusion was opened and stented, with a door to balloon time of 3 hours. 0 0 1 41 238 MMRF 1 1 278 14.0 So there is a definite inferior and lateral MI.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. A 99% LAD occlusion was stented. BP 110/67 HR 68 RR 14 (non-labored) SpO2 95 RA Physical exam revealed slight pallor and diaphoresis. Attached is the first ECG. 5] Walsh, B.
A mid-LAD culprit lesion was identified and stented. Cardiology felt her chest pain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution. References Naidu, S. American College of Cardiology.
American Heart Journal 170(6):1255-1264; December 2015. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent. Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. Derivation in LBBB: --> Smith SW.
It was opened and stented. 21, 2015 post by Dr. Smith ). Chest pain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated. The LAD was 100% occluded. Subsequent Peak cTnI was 46.84 ng/mL (consistent with LAD occlusion).
Dr. Smith illustrates how to measure these parameters with magnified views in his December 21, 2015 post. There was 100% occlusion of the RCA, which was stented. I describe and illustrate in detail my approach to incorporating these criteria in My Comment at the bottom of the December 16, 2019 post in Dr. Smiths ECG Blog.
In the present study, we investigated clinical and procedural characteristics predictive of MT success and failure.MethodsWe conducted a retrospective analysis of MT patients with LVO presenting to our academic comprehensive stroke center from 2015‐2020. Recanalization failure was defined as TICI 0‐2a and success as TICI 2b‐3.
Discharge ECG showed new Q wave and reperfusion TWI in III: Because the patient had the cath lab activated and received a stent, the discharge diagnosis was STEMI even though none of their ECGs met STEMI criteria. Troponin was 2,000 before cath but no subsequent troponin were done. This was STEMI(-)OMI.
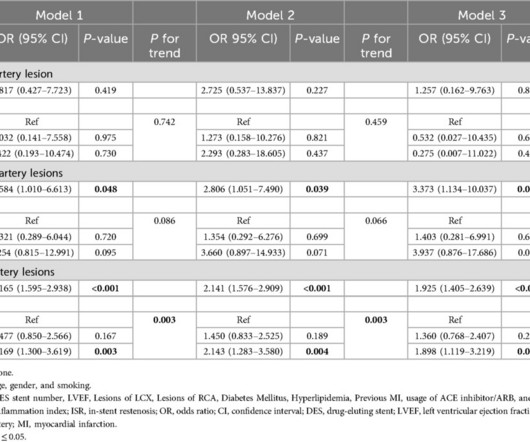
MethodsIn this retrospective cohort study, a total of 1,652 patients who underwent percutaneous coronary intervention (PCI) from February 2015 to December 2020 and were finally enrolled after follow-up with coronary angiography. The SII was calculated based on neutrophil, platelet and lymphocyte counts.
Current treatment is with anti-thrombotics and/or anticoagulation.Lesser option is to alter the flow disturbance caused by the web (surgery or stent). Ref : Berkhemer OA, Fransen PSS, Beumer D, et al; MR CLEAN Investigators. A randomized trial for intraarterial treatment for acute ischemic stroke. Christopher R. Reference 1.Rainer Rainer W.G.,
It was treated with a drug eluting stent. As per Hans Helseth ECG #1 clearly satisfies Modified Smith-Sgarbossa Criteria ( See My Comment in the December 16, 2019 post for my approach to incorporating these criteria and the December 21, 2015 post for illustration by Dr. Smith on how to measure these parameters ).
He eventually underwent CAG, where a circumflex occlusion was stented. Here is an old (2015), but still very relevant, lecture on T-wave inversion by Dr. Smith: 40 minute lecture on T-wave inversion Learning points : T-waves are often dynamic in ACS and may hint at reperfusion and re-occlusion before the ST-segment does.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content