This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int. Smith’s ECG Blog ).
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology. 2015 Oct; 66(4):355-362.
This is secondary to delayed postoperative cerebral ischemia and infarction caused by vasospasm.7 7 Clinical indicators like delirium can play a role in evaluating for delayed cerebral ischemia and infarction leading to timely management of vasospasms.5,8,9
Background:Myocardial infarction with nonobstructive coronary artery disease (MINOCA) is a special syndrome with clear evidence of myocardial ischemia, but no clear stenosis of coronary artery imaging sign. Circulation, Volume 150, Issue Suppl_1 , Page A4143007-A4143007, November 12, 2024.
However, despite successful recanalization, certain patients still experience large hemispheric ischemia (LHI), necessitating decompressive hemicraniectomy (DHC). These individuals were then matched into two groups: a study group who had undergone decompressive hemicraniectomy (38) and a control group of individuals who had not (79).
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. 2015, March 1). Chest trauma was suspected on initial exam. Here is his initial ECG around 1330: What do you think? Dyer From the Division of Cardiology, Thankavel, P. Myocardial contusion in an 8-year-old boy. Cramer, M.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
Lancet 2015 6. We are told that the Stress Echo that was performed showed objective evidence of inducible ischemia ( confirmed apparently by both wall motion abnormalities and ECG changes ). Was this objective evidence of inducible ischemia accompanied by chest pain? Am J Med 2021 5. Shah ASV, Anand A, Sandoval Y, et al.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This is the initial ECG: The QRS is widened with a regular cadence, and there are no discernable P waves.
So this relatively long QT interval is NOT due to ischemia but may be a result of CO Toxicity. Read more about CO poisoning and cardiac ischemia here (ECG is pasted below): What is the treatment for this subendocardial ischemia? Yelken B et al. Routine ECG recorded before hyperbaric therapy.Are they related?
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG. Also: As we always say, do not give morphine until you are committed to the cath lab. Clinical Cardiology, 45(4), 359–369. link] Macfarlane, P.
Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI. If you can safely and easily increase the patient's heart rate, you can convert the patient to sinus and repeat the ECG to see if the atrial repolarization wave was the cause of the concern for ischemia.
American Heart Journal 170(6):1255-1264; December 2015. EKG shown here: LAFB with no clear signs of OMI or ischemia. Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. Derivation in LBBB: --> Smith SW. No labs were performed. EKG and CT head were performed.
Chest pain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated. 21, 2015 post by Dr. Smith ). The average highest ST/S ratio in V1-V4 for a normal LBBB is about 0.11. is worrisome! The LAD was 100% occluded.
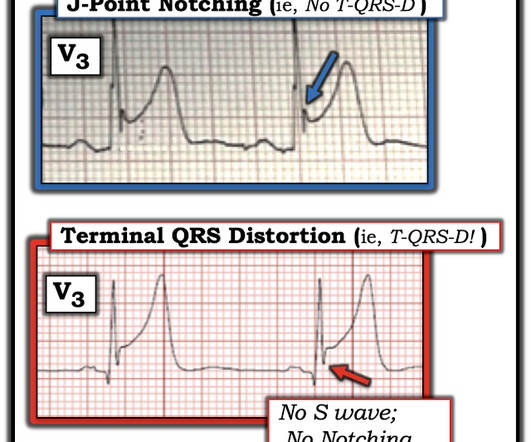
Terminal QRS distortion is present in anterior myocardial infarction but absent in early repolarization. American Journal of Emergency Medicine, 34 (11), 2182-2185. [4] 4] Baranchuk, A, et al. Differential diagnosis of rSr’ pattern in leads V1-V2: Comprehensive review and proposed algorithm. Annals of Noninvasive Electrocardiology, 20 (1), 7-17. [5]
Evidence of acute ischemia (may be subtle) vii. ST segment and T wave abnormalities consistent with or possibly related to myocardial ischemia. Annals of Emergency Medicine March 2015 ; Volume 65, Issue 3, Pages 268–276.e6 2nd or 3rd degree AV blocks or sinus pause of at least 2 seconds iv. Left BBB vi. Pathologic Q-waves viii.
His triage EKG is shown below: There is left bundle branch block, so the EKG must be evaluated for ischemia by Smith-modified Sgarbossa criteria. There is evidence of transmural ischemia of the posterior wall as well. Leads V1 to V4 have down-up shaped T waves typical of ischemia and atypical of LBBB.
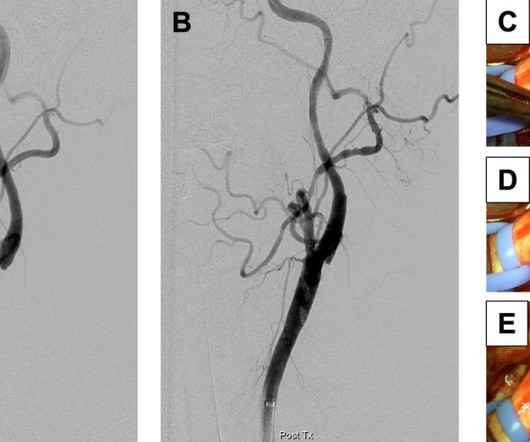
Management The web can create a flow disturbance, potentiating local thrombus formation, which can embolize producing resulting in cerebral ischemia. Fibromuscular hyperplasia of the carotid artery causing positional cerebral ischemia. Ref : Berkhemer OA, Fransen PSS, Beumer D, et al; MR CLEAN Investigators. Christopher R. Reference 1.Rainer
This case highlights how T-waves are very important in the assessment of ischemia and dynamic changes in acute coronary syndrome. I have often seen colleagues worry about T-wave inversions as a sign of ongoing ischemia. T-wave inversions in the acute phase of ACS are usually a welcome finding, indicating reperfusion.
The patient was started on heparin for possible NSTEMI vs demand ischemia. increasing stenosis, ischemia, volume changes, increased blood pressure, atrial fibrillation, etc.) The EKGs from the ED presentation were felt by cardiology to represent "subendocardial ischemia." Smith : these ECGs do NOT show subendocardial ischemia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content