This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. The American Journal of Emergency Medicine 2015; 33(6):786-790.
Whenever a patient does not have chestpain, the pre-test probability of OMI is diminished. Of course SOB, jaw pain, shoulder pain, etc can be a result of OMI, but the pretest probability is less and so you must scrutinize further. Here is the first ED ECG: COMPUTER INTERPRETATION: Electronic Atrial Pacemaker.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Isn't it amazing?? Don’t Ignore Bedside Echo Results! —
A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. Chestpain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Lancet 2015 6. Int J Cardiol 2013 2.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB. See text ). (
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. 2015 Nov;20(6):570-7. Does routine use of the 15-lead ECG improve the diagnosis of acute myocardial infarction in patients with chestpain? This case comes from Sam Ghali ( @EM_RESUS ). Thanks, Sam! This is his 12-Lead ECG: What do you think?
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
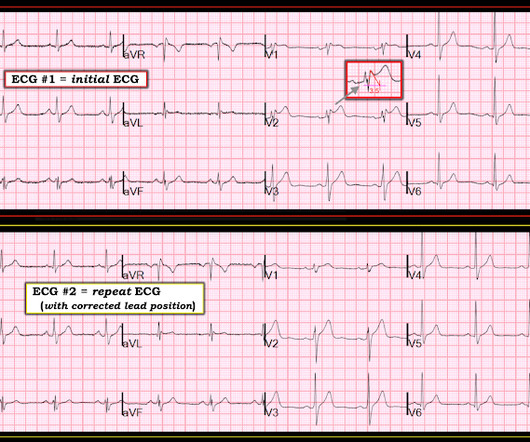
The cause of the abnormal baseline deflections seen in Figure-2 is most likely muscle tremor artifact ( See Bouthillet T — ACLS Med Training, Dec, 2015 ). Once the J-point is recognized in the chest leads ( RED arrows in leads V2,V3,V4 of Figure-2 ) — the marked ST elevation becomes obvious. He became unconscious on arrival.
As discussed in detail in ECG Blog #228 — this seemingly qualifies as a “ Silent ” MI ( Approximately half of those MIs not accompanied by CP — have some other associated symptom such as syncope, which substitutes as a “chestpain equivalent” ). What is M INOCA?
American Heart Journal 170(6):1255-1264; December 2015. Normal 0 false false false EN-US JA X-NONE Before the case, a few comments: Pendell and I just published a case report of a patient with left bundle branch block who presented with chestpain that then resolved. 0 0 1 41 238 MMRF 1 1 278 14.0
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
Diagnosis : Atrial flutter with 1:1 conduction, with fast AV conduction made possible by sympathetic drive of exercise On arrival, we obtained another 12-lead: Unremarkable Further history: One month history of shortness of breath on exertion, denies palpitations, chestpain, orthopnea, leg swelling.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. Below are two examples of this. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution. References Naidu, S. American College of Cardiology.
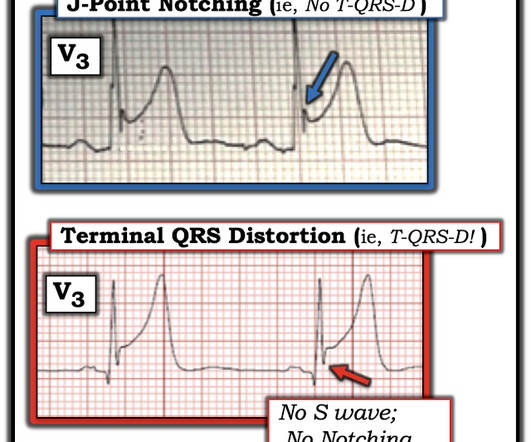
See this case of an awake patient without chestpain but with a CO level of 34%: CO poisoning. Figure-2: Comparison between ST elevation in lead V3 due to a repolarization variant ( TOP from the 4/27/2019 post) vs acute OMI ( BOTTOM from the 9/20/2015 post) , which manifests T-QRS-D ( See text ).
See these similar cases: A man in his sixties with chestpain Why is there inferior ST elevation, and would you get posterior leads? To the left of these tracings is schematic illustration of the Emery Phenomenon ( adapted from the 2015 post by Dr. Bojana Uzelac on Armel Carmona’s ECG Rhythms website ).
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. 2015 Oct; 66(4):355-362. This was contributed by some folks at Wake Forest: Jason Stopyra, Shannon Mumma, Sean O'Rourke, and Brian Hiestand. De Backer D et al.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. American Heart Journal 170(6):1255-1264; December 2015. Triage ECG: What do you think? This is diagnostic of proximal LAD occlusion.
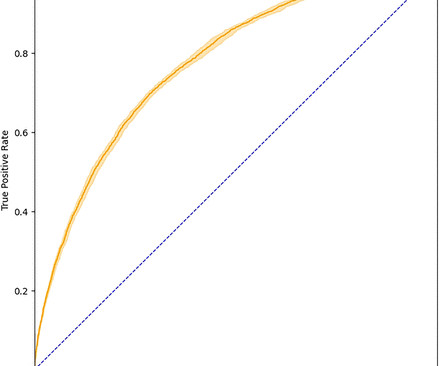
Introduction:Over 6 million patients (pts) present to US emergency departments annually with chestpain (CP), of which the majority are found to have no serious disease. Evaluation of these pts results in substantial costs for unnecessary hospitalization and extensive testing.
The quick and reliable prediction of troponin elevation for patients with chestpain from readily available ECGs may pose a valuable time-saving diagnostic tool during decision-making concerning this patient population. All patients had high-sensitivity troponin test results within 6 hours after 12-lead ECG.
Other trials that evaluated this subject were the WOEST trial (2013), Pioneer AF-PCI trial (2016), and ISAR-TRIPLE (2015). ACS QID 3103 A 64 year old Caucasian male with a history of extensive tobacco use, hypertension, hyperlipidemia, and obesity presents with acute onset chestpain. Incorrect Answers: A and E. Question 2.
A 50-something presented with epigastric and chestpain. Epigastric pain, Syncope, and Saddleback ST Elevation A 65 Year Old Man with Chestpain and Precordial ST Elevation Non-Vagal Syncope and Saddleback Morphology in V2 Is this STEMI? Here is his ECG: What do you think? QTc 388 ms. wave in V1??
She denied chestpain and denied feeling any palpitations, even during her triage ECG: What do you think? Her symptoms started suddenly about 48 hours ago, but had continued to worsen, including epigastric discomfort, nausea, cough, and dyspnea and lightheadedness on exertion.
Although in the context of chestpain such ST depression would be all but diagnostic of posterior OMI, one should make no conclusions in such an unusual case. Sci 5[4] 268-270, 2015 ) both highlight a likely association between acute development of ischemic J waves — and high risk of developing malignant ventricular arrhythmias.
the optimum QT correction formula for patients with chestpain was found to be unique for each individual ; it is a correction factor that can be calculated real-time for each patient by taking multiple measurements over a range of heart rates. Acad Emerg Med 2015 Oct; 22(10):1139-44. In this study by Hasanien et al. ,
Patient 2 : 55 year old with 5 hours of chestpain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This was missed by the treating physician, but the chestpain resolved with aspirin.
He contacted EMS due to acute onset chestpain and feeling unwell and fatigued. He subsequently developed worsening chestpain. This, in the context of worsening chestpain , is evidence of reocclusion of the infarct-related artery and active OMI in development. See this case: A man his 50s with chestpain.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Annals of Emergency Medicine March 2015 ; Volume 65, Issue 3, Pages 268–276.e6
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
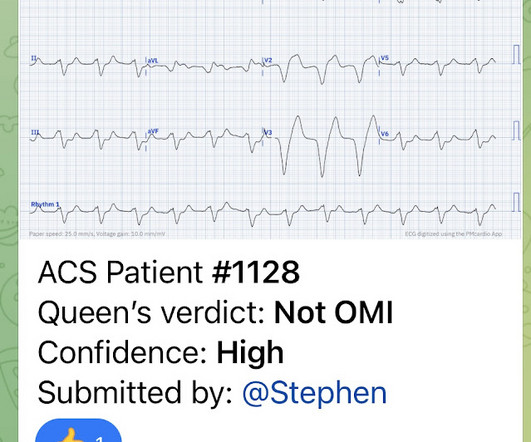
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chestpain at 2343. It is awaiting FDA approval (but approved for 1.5 There is ST elevation in the inferior leads. The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent").
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content