This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
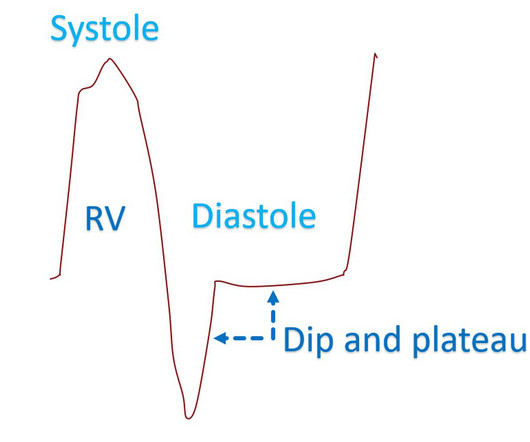
It is mentioned that square root sign can also occur in right right ventricular cardiomyopathy and severe bradycardia [1]. 2015 Mar-Apr;67(2):175-82. Epub 2015 May 13. Reference Doshi S, Ramakrishnan S, Gupta SK. Invasive hemodynamics of constrictive pericarditis. Indian Heart J. doi: 10.1016/j.ihj.2015.04.011. 2015.04.011.
The American Journal of Emergency Medicine 2015; 33(6):786-790. Electrocardiographic Criteria to Differentiate Acute Anterior ST Elevation Myocardial Infarction from Left Ventricular Aneurysm. link] So I responded with these words: Smith : "There are QS waves, which suggest old MI. But the T-waves in LV aneurysm are not this big.
2015, March 1). Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). Dyer From the Division of Cardiology, Thankavel, P.
Abstract Introduction Severe transitory episodes of bradycardia with subsequent syncope in children are common, and generally portend a benign prognosis. Patients with SP or AVB, 21 years of age or younger, who underwent CNA between 2015 and 2021 were included. Methods This is a single-center, case series study. The median age was 18.9
Athlete’s bradycardia due to increased parasympathetic tone and decreased sympathetic tone is a well-known observation. Though sinus bradycardia is usual, other abnormalities like sinus arrhythmia, sinus arrest, wandering atrial pacemaker and coronary sinus rhythm have been described. 2015 Apr;16(4):353.
Sci 5[4] 268-270, 2015 ) both highlight a likely association between acute development of ischemic J waves — and high risk of developing malignant ventricular arrhythmias. Rituparna et al — as well as Chauhan and Brahma ( Int.
After the heart rate increased slightly, here was the repeat ECG: Sinus bradycardia, only slightly faster rate than prior. To the left of these tracings is schematic illustration of the Emery Phenomenon ( adapted from the 2015 post by Dr. Bojana Uzelac on Armel Carmona’s ECG Rhythms website ).
Patient 2 : 55 year old with 5 hours of chest pain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Smith : The fact that the ECG did not evolve is further proof that this was the baseline ECG.
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content