This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Methods This study included consecutive patients with iSTEMI treated with percutaneous coronary intervention (PCI) between 1 January 2011 and 15 July 2019 at a single, tertiary referral centre.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes. The case continues. Kontos, M.
IntroductionHypoxic liver injury (HLI) and Killip classification are poor prognostic factors in patients with ST-segment elevation myocardial infarction (STEMI). Early recognition of HLI and accurate assessment of Killip classification is warranted for effective management of STEMI.
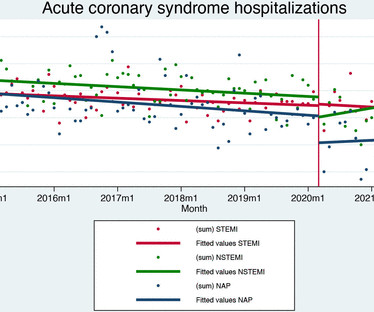
Methods and results Data for all patients admitted to hospital care for acute coronary syndromes in Slovenia (nationwide cohort) between 2014 and 2021 were obtained by merging the national hospital database, national medicines reimbursement database and population mortality registry using unique identifying numbers.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. These include: i ) appreciation of how problematic the definition of “acute STEMI” can be; and , ii ) illustration of how dependence on this definition may result in overlooking acute coronary occlusion. Thelin et al.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. She was out walking her dog when she developed sudden dizziness and light-headedness. When EMS found her, she was dyspneic and diaphoretic.
LVH and the diagnosis of STEMI - how should we apply the current guidelines? Journal of Electrocardiology 47 (2014) 655–660. This one mimics inferior STEMI (Figure 4): Concentric LVH, NO wall motion abnormality Case 5. How about diagnosing anterior STEMI in the setting of LVH? All troponins were negative.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI. It is not a missed STEMI, but it is a missed coronary occlusion. The peak troponin I was over 100.
Another overlooked OMI ( Cardiologist limited by STEMI Definition — OMI evident by Mirror Test ) — See My Comment at the bottom of the page in the September 21, 2020 post on Dr. Smith’s ECG Blog. Smith’s ECG Blog. ECG Media Pearl # 9 ( 5:40 minutes Video ) — ECG Blog #192 — Reviews the 3 Causes of AV Dissociation ( 2/9/2021 ).
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI). This is from the 2014 ACC/AHA guidelines. The troponin I returned at 4.1 mm STE in one lead.
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. A DDENDUM ( 8/3/2024 ) : In the following 5 Figures — I post written summary from my ECG-2014-ePub on the ECG diagnosis of A cute P ericarditis. Pericarditis maybe."
Prehospital ECG: Obvious anterolateral STEMI (Proximal LAD occlusion) The cath lab was activated prehospital by the medics. Interventionalist at the Receiving Hospital: "No STEMI, no cath. Here is one case of a patient I saw. He was a 30-something with chest pain. A male in his 30's complained of sudden severe substernal chest pain.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
This blog post reviews the basics for predicting the " C ulprit" A rtery — as well as the importance of the term, " O MI" ( = O cclusion-based MI ) as an improvement from the outdated STEMI paradigm. ECG Blog #294 — How to tell IF the "culprit" artery has reperfused. ECG Blog #194 — AIVR as a sign that the "culprit" artery has reperfused.
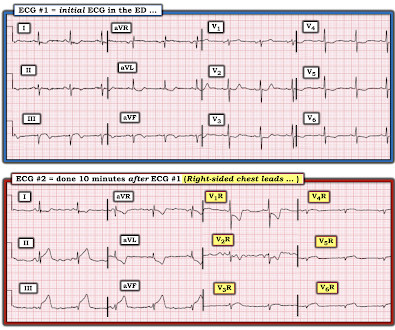
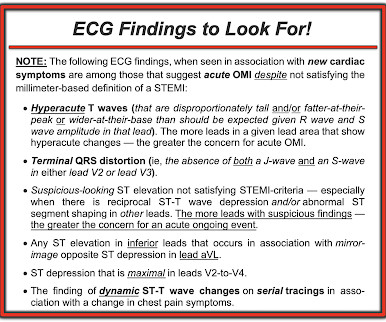
To EMPHASIZE: Despite there not being "enough" ST elevation to satisfy millimeter-based criteria for an acute "STEMI" in ECG #1 — this initial ECG is absolutely diagnostic of OMI. The surprisingly tall terminal T wave positivity that we see in lead V2 almost certainly represents reperfusion in the posterior wall distribution.
ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. Section 2F ( 6 pages = the " short " Answer ) from my ECG-2014 Pocket Brain book provides quick written review of the AV Blocks.
Here is the Queen of Heart's interpretation: The cath lab had been activated for concern of STEMI. Learning Points: This is one of many examples of false positive STEMI criteria, which is distinguishable by expert humans, and now by AI such as QOH. No prior ECG was available.
But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. Still no WPW pattern, and more obvious inferoposterior OMI, but still STEMI negative. CMAJ 2014. The emergency physician wasn’t sure what to make of the changes from one ECG to the next but was concerned about ACS.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. KEY Point: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern ( World J Cardiol 6(3):81-86, 2014 ).
Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria. As has been mentioned numerous times on this site and is redemonstrated here: expert, subjective ECG interpretation is superior to STEMI criteria. Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease. What do you see?
He commented: "by every measure, this would be RBBB with inferior and lateral STE appearing to be STEMI," but he also noted that there are several features that appear similar to false positives (like the first case above). There is also much STE in V3-V6, especially V4-V6, that must be considered to be STEMI. Peak troponin was 3.21
ECG Blog #193 — for review of the concept of “OMI” ( = O cclusion-based M yocardial I nfarction ) — and why this term should replaced the outdated STEMI paradigm. ECG Blog #337 and ECG Blog #294 — relevant related Blog posts on the importance of the OMI paradigm ( in preference to the outdated STEMI paradigm ). =
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Case Rep Emerg Med 2014 7. Patel J, Alattar F, Koneru J, et al.
OMI that are not STEMI can be very subtle and difficult to diagnose even though the findings are very specific. With a little bit of practice — it becomes EASY to recognize the "shelf-like" ( flat ) shape of ST depression — that looks like a stemi when this image is inverted.
Cases of acute MI that were initially misdiagnosed as myo- or peri-carditis: 24 yo woman with chest pain: Is this STEMI? I excerpted Figure-2 from Section 12 on Pericarditis , from my ECG-2014-ePub. Figure-2: Spodick's Sign — excerpted from Grauer K, ECG-2014-ePub ( See Text ). What happens then? Pericarditis?
Here is data from a study we published in 2014 for type II NonSTEMI: Sandoval Y. Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. First was 2.9 ng/mL and subsequentle dropped to 1.5 ng/mL Such high troponin I is very unusual in type 2 MI. Murakami M.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." of very high risk NSTEMI patients underwent angiography in less than 2 hours in accordance with the 2014 ACC/AHA guidelines. How does the Queen of Hearts do? In fact, in the one study I'm aware of in which it has been studied, only 6.4%
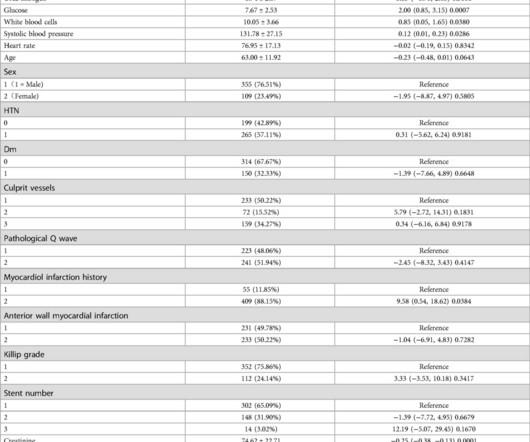
BackgroundAcute myocardial infarction (AMI), particularly ST-segment elevation myocardial infarction (STEMI), significantly impacts global health, exacerbated by risk factors such as diabetes mellitus (DM). This study highlights the importance of comprehensive FBG monitoring and management to improve outcomes for STEMI patients.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
PEARL # 3: Knowing there is an acute inferior STEMI I looked next to see if there is also acute posterior involvement ( which so often accompanies inferior MI ). But larger-than-expected Q waves in each of the inferior leads ( especially in lead III ) are probably the result of this patients ongoing acute inferior STEMI.
At 1210, the case was discussed with a cardiologist at a PCI capable facility, who accepted the patient for transfer, noting the ST depression in anterior leads as consistent with ischemia but not a STEMI. Figure-2: Illustration of the rational for the Mirror Test ( Figure excerpted from Grauer K: ECG-2014 Pocket Brain ePub ). =
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! HyperKalemia with Cardiac Arrest. References 1. Lindner et al. Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: Improving Global Outcomes conference.
Or, there could be mid-ventricular Takotsubo , in which there is poor function ( and ballooning ) o f the mid-LV, with good function at both the base and the apex and, still other anatomic possibilities ( See the June 24, 2014 post and My Comment in the July 21, 2022 post of Dr. Smith's ECG Blog regarding Takotsubo variant patterns ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content