This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
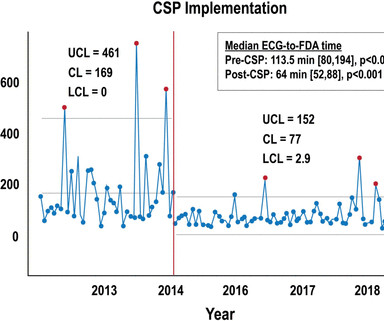
Key metrics and clinical outcomes were compared before and after CSP implementation. Methods This study included consecutive patients with iSTEMI treated with percutaneous coronary intervention (PCI) between 1 January 2011 and 15 July 2019 at a single, tertiary referral centre.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." 2014 AHA/ACC guideline for the management of patients with non–ST-elevation acute coronary syndromes. The case continues. Kontos, M.
LVH and the diagnosis of STEMI - how should we apply the current guidelines? Journal of Electrocardiology 47 (2014) 655–660. This one mimics inferior STEMI (Figure 4): Concentric LVH, NO wall motion abnormality Case 5. How about diagnosing anterior STEMI in the setting of LVH? For details, read this post.
His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI. It is not a missed STEMI, but it is a missed coronary occlusion. The peak troponin I was over 100.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
Here is the Queen of Heart's interpretation: The cath lab had been activated for concern of STEMI. Other outcome information is not available. Learning Points: This is one of many examples of false positive STEMI criteria, which is distinguishable by expert humans, and now by AI such as QOH. No prior ECG was available.
Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria. As has been mentioned numerous times on this site and is redemonstrated here: expert, subjective ECG interpretation is superior to STEMI criteria. Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." of very high risk NSTEMI patients underwent angiography in less than 2 hours in accordance with the 2014 ACC/AHA guidelines. Unfortunately, no futher outcome is known (echo, survival, etc.) How does the Queen of Hearts do? Lupu et al.
BackgroundAcute myocardial infarction (AMI), particularly ST-segment elevation myocardial infarction (STEMI), significantly impacts global health, exacerbated by risk factors such as diabetes mellitus (DM). This study highlights the importance of comprehensive FBG monitoring and management to improve outcomes for STEMI patients.
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: Improving Global Outcomes conference. HyperKalemia with Cardiac Arrest. References 1.
Was her outcome to be expected for ostial RCA OMI? Note characteristic ballooning of the apex and hypercontractility of the base during cardiac cath ( Figure excerpted from Grauer K: ECG-2014- Expanded ePub, KG/EKG Press ). = The patient certainly had OMI and received treatment for it. We will never know for certain. link] Bentzon, J.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content