This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
There may be ischemia present, but it is not evident on the ECG. LVH and the diagnosis of STEMI - how should we apply the current guidelines? LVH and the diagnosis of STEMI - how should we apply the current guidelines? Journal of Electrocardiology 47 (2014) 655–660. All troponins were negative. Birnbaum Y and Mahboob A.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR.
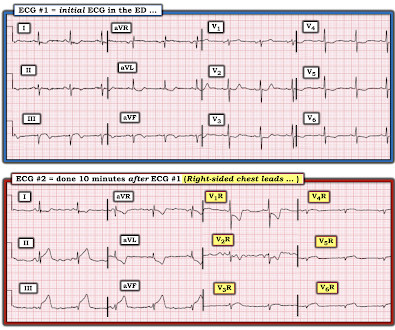
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF. Thelin et al.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. That said — I did not interpret these differences as the result of acute ischemia. Of note, there is arguably terminal QRS distortion in V4-V6. Pericarditis maybe."
Prehospital ECG: Obvious anterolateral STEMI (Proximal LAD occlusion) The cath lab was activated prehospital by the medics. Perhaps they indicate an open artery with minimal flow and severe subendocardial ischemia, but not total subepicardial ischemia. Interventionalist at the Receiving Hospital: "No STEMI, no cath.
This blog post reviews the basics for predicting the " C ulprit" A rtery — as well as the importance of the term, " O MI" ( = O cclusion-based MI ) as an improvement from the outdated STEMI paradigm. ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. Still no WPW pattern, and more obvious inferoposterior OMI, but still STEMI negative. 2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia.
To EMPHASIZE: Despite there not being "enough" ST elevation to satisfy millimeter-based criteria for an acute "STEMI" in ECG #1 — this initial ECG is absolutely diagnostic of OMI. ECG Blog #184 and ECG Blog #167 — illustrate the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Case Rep Emerg Med 2014 7. Patel J, Alattar F, Koneru J, et al.
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. There is also much STE in V3-V6, especially V4-V6, that must be considered to be STEMI. The challenge is magnified when trying to assess BBB tracings for acute ischemia.
Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? This is most consistent with ischemia/infarction in the distribution of the left circumflex coronary artery. non-occlusive ischemia) 2. Thus, they have much less voltage. They have ZERO ST Elevation.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. KEY Point: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern ( World J Cardiol 6(3):81-86, 2014 ).
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. Here is data from a study we published in 2014 for type II NonSTEMI: Sandoval Y.
It is not clear by her note what she meant by this (whether or not she recognized this EKG as diagnostic of transmural ischemia, and if so, of what territory) but emergent reperfusion therapy was not pursued. Subendocardial ischemia does not localize. At 1022, a troponin I (ref range <0.034 ng/mL) resulted at 4.437 ng/mL.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
PEARL # 3: Knowing there is an acute inferior STEMI I looked next to see if there is also acute posterior involvement ( which so often accompanies inferior MI ). But larger-than-expected Q waves in each of the inferior leads ( especially in lead III ) are probably the result of this patients ongoing acute inferior STEMI.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content