This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
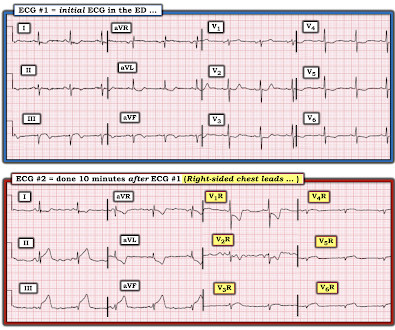
That said — the ECG in Figure-1 should prompt the following considerations: The symmetric chest lead T wave inversion in ECG #1 could be a sign of coronary disease, potentially with acute ischemia. ECG Blog #209 — Reviews the ECG diagnosis of Wellens’ Syndrome ( What it is — and what it is not! ).
There may be ischemia present, but it is not evident on the ECG. Journal of Electrocardiology 47 (2014) 655–660. This patient with LVH had chest pain ( Figure 7 ) LVH with ST-T abnormalities with superimposed ischemia. LVH and the diagnosis of STEMI - how should we apply the current guidelines?
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI. Circulation 2014 2. link] References 1. Amsterdam et al.
This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. EKG 3 is diagnostic for developing re-occlusion, and EKG 4 proves that the nitrates relieved the ischemia. = This proves effective treatment of the recurrent ischemia." Buller, C. Starovoytov, A., Robinson, S.,
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
As a result — IF no "fixable" cause is found ( ie, ischemia/infarction — electrolyte disturbance — rate-slowing medication ) — then because of the AV block and very slow heart rate, this patient will probably need a pacemaker. There are also twice as many P waves as QRS complexes — so at the least, there is 2nd-degree AV block.
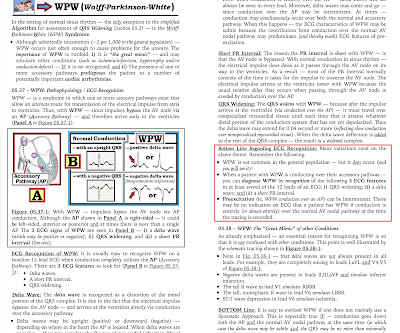
N OTE : In the A ddendum below — I've reproduced in Figures-4 , -5 , -6 and -7 ( from my ECG-2014-ePub ) — those Sections that review the basics for ECG diagnosis of WPW — and — assessment of the common arrhythmias expected with WPW. ECG Blog #157 — Can you diagnose ischemia and/or infarction when there is WPW?
That said — I did not interpret these differences as the result of acute ischemia. A DDENDUM ( 8/3/2024 ) : In the following 5 Figures — I post written summary from my ECG-2014-ePub on the ECG diagnosis of A cute P ericarditis. A more likely reason is the change in QRS morphology in the precordial leads.
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. non-occlusive ischemia) JAHA 2021 3. -- Meyers HP, Bracey A, Lee D, et al.
2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia. 3] So a patient with WPW can have the pattern induced by ischemia, and there is also a report of a patient with pre-existing WPW which was “ablated” by myocardial infarction after an LAD occlusion.[4]
Case Rep Emerg Med 2014 7. We are told that the Stress Echo that was performed showed objective evidence of inducible ischemia ( confirmed apparently by both wall motion abnormalities and ECG changes ). Was this objective evidence of inducible ischemia accompanied by chest pain? Lancet 2015 6.
FOR O ther E xamples of Acute RV MI: Discussion of the 12-lead ECG in Blog #187 — See Figure-4 in ECG Blog #80 ( More on the "culprit" artery in this post ) — See ECG Blog #141 — Figure-5 ( together with Figure-6 ): Reviews the ECG Essentials of RV MI ( Excerpted from my ECG-2014-ePub ).
Echo immediate: 35% EF with anterior, septal, and apical wall motion abnormalities Echo convalescent, 2 months later: Better, with EF up to 45-50% I posted this in 2014: Is the LAD really completely occluded when there are de Winter's waves? Peak troponin I (contemporary) was 101.0
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
However, its refined version LMWH, though made it more palatable & user friendly, it un-apologetically took the sting out of regular heparin, made it less efficacious (more glamorous though) LMWH usage is in CAD widespread , it has suspect value* in true ongoing ischemia in any active ACS situation. 2014 Sep;19(5):451-6.
ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
She requires maximal medical management per all current guidelines (including heparin and P2Y12 inhibitor per cardiology), as well as consideration for emergent cath in the case of persistent ischemia. So what will you do for this patient? They found an acute, total, thrombotic occlusion of the proximal LAD. They opened it. Patel et al.,
Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? This is most consistent with ischemia/infarction in the distribution of the left circumflex coronary artery. non-occlusive ischemia) 2. Thus, they have much less voltage. They have ZERO ST Elevation.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. Here is data from a study we published in 2014 for type II NonSTEMI: Sandoval Y.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! The note also says "slight lateral ST elevations noted, likely early repolarization since unchanged compared to 2014." Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG.
This suggests ischemia of uncertain duration. Section 2F ( 6 pages = the " short " Answer ) from my ECG-2014 Pocket Brain book provides quick written review of the AV Blocks. This means that we can assess ST-T wave morphology for ischemic changes in simultaneously-recorded leads V1,V2,V3 for beat #5 — and in leads V4,V5,V6 for beat #7.
This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. It appears that on occasion — J waves may be induced by ischemia ( thought to reflect an acute injury current from impending myocardial infarction ). But maybe not. Thelin et al.
It is not clear by her note what she meant by this (whether or not she recognized this EKG as diagnostic of transmural ischemia, and if so, of what territory) but emergent reperfusion therapy was not pursued. Subendocardial ischemia does not localize. At 1022, a troponin I (ref range <0.034 ng/mL) resulted at 4.437 ng/mL.
Many patients suffer from a systemic inflammatory response and local myocardial ischemia after off-pump coronary artery bypass grafting, which is related to an adverse prognosis. BackgroundA pathological decrease in the serum prealbumin level is closely associated with the severity of various diseases and complications after surgery.
But it also shows a massive area of total ischemia in the LAD territory: CT shows the infarct The CT is with contrast, which increases density (which looks more white). Most dissections which cause coronary ischemia are into the RCA ostium ("ostium" = locations of takeoff of the vessel). No ECG was recorded after pain resolution.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Here is the final angiogram following placement of a stent in the ostial RCA. Journal of Geriatric Cardiology , 19 (6).
Section 2F ( 6 pages = the " short " Answer ) from my ECG-2014 Pocket Brain book provides quick written review of the AV Blocks ( This is a free download ). ECG Blog #184 illustrates the " m agical" m irror- i mage o pposite relationship with acute ischemia between lead I II and lead a VL.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content