This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
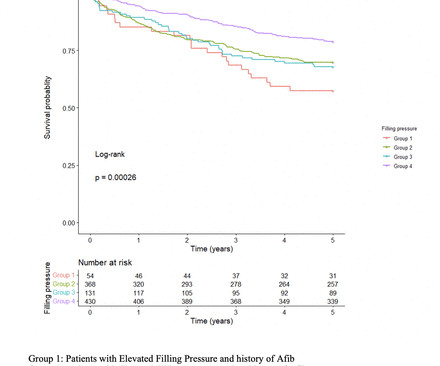
However, the impact of elevated FP as detected by pretranscatheter aortic valve replacement (TAVR) echocardiogram on long-term outcomes after TAVR remains unclear. Methods This was a retrospective study of all patients who underwent TAVR between 1 January 2014 and 31 December 2017. Patients with elevated FP had a mean age of 81.2±8.6
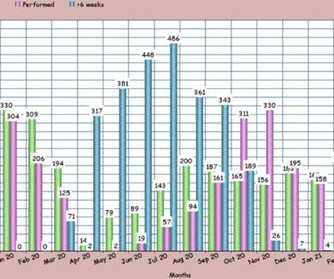
males), referred for a stress echocardiogram (SE), who underwent ESE between July 2020 (immediate post lockdown) and January 2021 according to national safety guidelines, in addition to patients wearing masks during ESE. Methods and results Baseline data were collected prospectively on 740 consecutive patients (mean age 61.4
Methods A cross-sectional screening study was conducted between 2014 and 2016. Echocardiograms were performed with a standardised image acquisition protocol and reported by cardiologists. Echocardiograms were performed with a standardised image acquisition protocol and reported by cardiologists.
Results There were 664 patients who had an index HF admission to John Hunter and Tamworth hospitals in 2014. In terms of HF type, 29% had HFrEF, 37% had HFpEF, while the remainder (34%) did not have an echocardiogram within 1 year of admission and could not be classified. The median follow-up was 3.3
For instance, the average waiting time for an echocardiogram at Turin’s Molinette Hospital was 31 days in 2016 and an even longer 53 days for a Holter ECG. Prior to the new regulation, getting a consultation with a cardiologist or getting a needed diagnostic cardiology test often involved long waiting times.
On echocardiogram, there was a 40% ejection fraction with anterior wall motion abnormality. Am Heart J December 2014; 168:884-90. == MY Comment , by K EN G RAUER, MD ( 12/6 / 2023 ): == Even a decade ago — Dr. Smith was already convincingly diagnosing acute OMIs, as per his discussion above. The peak troponin I was over 100.
Echocardiogram: The estimated left ventricular ejection fraction is 34% Regional wall motion abnormality-lateral, akinetic. Figure-1: Illustration of the rational for the Mirror Test ( Figure excerpted from Grauer K: ECG-2014 Pocket Brain ePub ). A massive acute OMI.
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. 10 The 2014 ACC/AHA guidelines for the Management of Patients with Valvular Heart Disease , referencing this article, gives this recommendation: "CLASS IIb 1. Heart 2011; 97 : 838-843 [link] 14.
See this case: what do you think the echocardiogram shows in this case? Methods STEMI activations between January 2014 and April 2018 at the University of Arizona Medical Center were identified. POCUS showed good LV-function and no pericardial effusion. The patient had mild but diffuse abdominal tenderness.
No further echocardiograms were available after cath. The patient was discharged one day after intervention and appears to be doing well. The full thickness infarction with LV aneurysm morphology places him at a higher risk for short and long term complications (e.g.,
Both the outdated 2014 AHA/ACC guidelines and the updated 2023 ESC guidelines recommend immediate invasive management of patients with uncontrolled chest pain. Her contrast enhanced echocardiogram is shown below in the parasternal short axis view. The patient suffered a large infarct. Kontos, M. Levine, G. Liebson, P. Mukherjee, D.,
Formal echocardiogram showed normal EF, no wall motion abnormalities, no pericardial effusion. KEY Point: A number of conditions other than Brugada Syndrome may temporarily produce a Brugada-1 ECG pattern ( World J Cardiol 6(3):81-86, 2014 ). No more troponins were done. He was found to be influenza positive.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content