This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
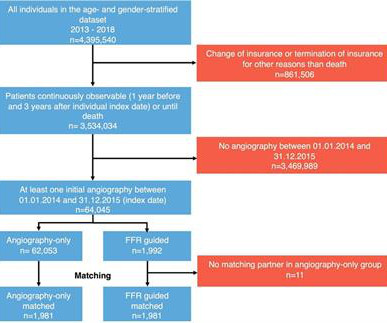
Patients undergoing coronary angiography between January 2014 and December 2015 were included in the analysis. Eligible patients had at least one inpatient coronaryangiogram for suspected coronary artery disease between January 2014 and December 2015.
All patients had CT coronaryangiograms at the start of the study and repeated after about one year. 4 Coronary atheroma regression and plaque characteristics assessed by grayscale and radiofrequency intravascular ultrasound after aerobic exercise. 2014 Nov 15;114(10):1504-11. Sci Rep 11 , 7999 (2021). Am J Cardiol.
Hospital evaluation for this patient was negative for an acute coronary syndrome ( ie, CT coronaryangiogram was normal — troponin was not elevated — and Echo was negative, with no sign of pericardial effusion ). CT CoronaryAngiogram showed no sign of underlying coronary disease.
Like they would for any other acute arterial occlusion syndrome (such as suspicion of acute large vessel stroke), they take the patient across the hall and perform an immediate CT (coronary) angiogram, showing patent coronaries. An emergent echo also confirms no regional wall motion abnormality.
The diagnostic coronaryangiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease. Heart 2011; 97 : 838-843 [link] 14.
We investigated the incidence of an acutely occluded coronary in patients presenting with STE-aVR with multi-lead ST depression. Methods STEMI activations between January 2014 and April 2018 at the University of Arizona Medical Center were identified.
Heitner et al found that in 14% of patients with NSTEMI, a blinded interventional cardiologist interpreting coronaryangiograms identified a different culprit artery than CMR ( [link] ). Figure-2: Illustration of the rational for the Mirror Test ( Figure excerpted from Grauer K: ECG-2014 Pocket Brain ePub ). =
Angiogram Door to balloon time was 120 minutes (much too long) because of time taken for a CT. Coronaryangiogram showed 100% mid LAD occlusion for which she received a DES with excellent angiographic result. It was not SCAD (coronary dissection) Highest troponin I was 37,000 ng/L, but it was not measured to peak.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content