This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A middle aged male presented with chestpain. There may be ischemia present, but it is not evident on the ECG. Journal of Electrocardiology 47 (2014) 655–660. In LVH, T-wave inversions are usually much more assymetric , like these (Figure 2): Acute Chestpain, but baseline ECG. All troponins were negative.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. 2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Case Rep Emerg Med 2014 7.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. 2014 AHA/ACC guideline for the management of patients with non-ST elevation acute coronary syndromes.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. That said — I did not interpret these differences as the result of acute ischemia. A DDENDUM ( 8/3/2024 ) : In the following 5 Figures — I post written summary from my ECG-2014-ePub on the ECG diagnosis of A cute P ericarditis.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
The ECG in Figure-1 was obtained from a man in his mid-60s — who presented with new chestpain. The magnitude of ST-T wave change is maximal in lead V2 — with the insert in this lead showing a positive "Mirror" Test — that in this patient who presents with new chestpain, is diagnostic of acute posterior OMI — until proven otherwise.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
But, in a patient who presents to the ED for new chestpain — seeing these subtle findings that are localized to leads V2- thru -V4 should at the least make you consider acute posterior OMI ( O cclusion-based MI ) — until you prove otherwise. To EMPHASIZE: These are subtle findings. What do YOU think?
He was a 30-something with chestpain. Echo immediate: 35% EF with anterior, septal, and apical wall motion abnormalities Echo convalescent, 2 months later: Better, with EF up to 45-50% I posted this in 2014: Is the LAD really completely occluded when there are de Winter's waves? Here is one case of a patient I saw.
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. As a result — IF no "fixable" cause is found ( ie, ischemia/infarction — electrolyte disturbance — rate-slowing medication ) — then because of the AV block and very slow heart rate, this patient will probably need a pacemaker.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. Here is data from a study we published in 2014 for type II NonSTEMI: Sandoval Y.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. Back to the case: The providers recognized persistent ischemia and likely occlusion, and discussed this with cardiology who took the patient immediately for cath. They opened it.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history? J Electrocardiol 2013;46:240-8 2.
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chestpain. Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? non-occlusive ischemia) 2.
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
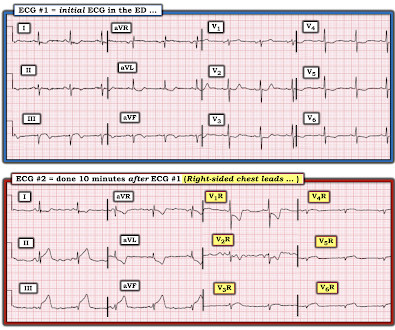
This suggests ischemia of uncertain duration. Section 2F ( 6 pages = the " short " Answer ) from my ECG-2014 Pocket Brain book provides quick written review of the AV Blocks. This means that we can assess ST-T wave morphology for ischemic changes in simultaneously-recorded leads V1,V2,V3 for beat #5 — and in leads V4,V5,V6 for beat #7.
This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. It appears that on occasion — J waves may be induced by ischemia ( thought to reflect an acute injury current from impending myocardial infarction ). But maybe not. Thelin et al.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. No ECG was recorded after pain resolution. He had never experienced a similar pain at rest or upon exertion.
A 62 year old man with hyperlipidemia presented to a rural emergency department with 7 hours of 3/10 chestpain. It is not clear by her note what she meant by this (whether or not she recognized this EKG as diagnostic of transmural ischemia, and if so, of what territory) but emergent reperfusion therapy was not pursued.
The ECG in Figure-1 was obtained from a middle-aged man who presents to the ED ( E mergency D epartment ) with 6 hours of chestpain. Figure-1: The initial ECG in today's case obtained from a middle-aged man with 6 hours of chestpain. ( He is hemodynamically stable. ECG Blog #228 Reviews the concept of " Silent " MI.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. link] Bentzon, J.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content