This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. This is from the 2014 ACC/AHA guidelines. It was not relieved by anything.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. CMAJ 2014. Additional Examples of OMI with WPW: CLICK HERE — for a similar case of a patient with WPW and new-onset chestpain.
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Anxiety is a common cause of chestpain with tachycardia.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Case Rep Emerg Med 2014 7.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
He presented to the ED because he developed sudden severe, sharp, pleuritic (but not positional), substernal and left mid to lower chestpain. Another similar case: Teenager with chestpain and slightly elevated troponin. I excerpted Figure-2 from Section 12 on Pericarditis , from my ECG-2014-ePub. Pericarditis?
See this case: Persistent ChestPain, an Elevated Troponin, and a Normal ECG. This is different from nitroglycerin which produces vasodilation and can improve by pain improving myocardial perfusion. You do not need to be better than the Queen of Hearts at EKG to understand that refractory chestpain NEEDS CATH NOW.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. 2014 AHA/ACC guideline for the management of patients with non-ST elevation acute coronary syndromes.
Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. A DDENDUM ( 8/3/2024 ) : In the following 5 Figures — I post written summary from my ECG-2014-ePub on the ECG diagnosis of A cute P ericarditis. I sent this to our group without information and Dr. Smith responded: "Not OMI.
Methods Patients with a first episode of acute pericarditis were consecutively enrolled between January 2014 and June 2022, and divided into four groups according to age (G1: 18–35 years; G2: 35–55 years; G3: 55–75 years; G4: >75 years). Results A total of 471 patients (median age 56.3 (IQR IQR 33–73) years, 32.3%
The ECG in Figure-1 was obtained from a man in his mid-60s — who presented with new chestpain. The magnitude of ST-T wave change is maximal in lead V2 — with the insert in this lead showing a positive "Mirror" Test — that in this patient who presents with new chestpain, is diagnostic of acute posterior OMI — until proven otherwise.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
A middle aged male presented with chestpain. Journal of Electrocardiology 47 (2014) 655–660. In LVH, T-wave inversions are usually much more assymetric , like these (Figure 2): Acute Chestpain, but baseline ECG. Here is another patient with severe LVH who presented with chestpain and ruled out for MI.
On occasion — such anterior lead ST elevation ( instead of T wave inversion ) can be seen with acute PE ( Zhan et al — Ann Noninvasive Electrocardiol 19(6):543-551, 2014 — and — Omar HR — Eur Heart J: Acute Cardiovascu Care (5(8): 579-586, 2016 ). Figure-8: Summary of KEY findings in the ECG diagnosis of acute PE ( from my ECG-2014-ePub ).
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
But, in a patient who presents to the ED for new chestpain — seeing these subtle findings that are localized to leads V2- thru -V4 should at the least make you consider acute posterior OMI ( O cclusion-based MI ) — until you prove otherwise. To EMPHASIZE: These are subtle findings. What do YOU think?
Methods This study included consecutive patients with iSTEMI treated with percutaneous coronary intervention (PCI) between 1 January 2011 and 15 July 2019 at a single, tertiary referral centre.
. = M Y T houghts on the ECG in Figure-1: It's important to remember that the ECG in Figure-1 was obtained from a previously healthy 30-ish year old man who presented with an episode of vasovagal syncope — but there is no mention of chestpain in the history ! B OTTOM L ine : Need for Transfer to a PCI-capable Center?
He was a 30-something with chestpain. Echo immediate: 35% EF with anterior, septal, and apical wall motion abnormalities Echo convalescent, 2 months later: Better, with EF up to 45-50% I posted this in 2014: Is the LAD really completely occluded when there are de Winter's waves? Here is one case of a patient I saw.
But the History in today's case was acute shortness of breath with dizziness and lightheadedness — and, essentially without chestpain! Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
Here is data from a study we published in 2014 for type II NonSTEMI: Sandoval Y. At some point he returned with chestpain, and all these findings were put into place. Many MI do not have chestpain 4. Of this group (ie, which is comprised of >1/4 of all MIs ) — about HALF have NO chestpain at all.
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. Usefulness of automated serial 12-lead ECG monitoring during the initial emergency department evaluation of patients with chestpain. Ann Emerg Med 1998;31(1):3-11. Wang T, Zhang M, Fu Y, et al. Marti D et al.
No chestpain. In a previously healthy adolescent ( who is 15 years old in today's case ) — the presentation of an acute febrile illness that is without a complaint of chestpain, is highly unlikely to be due to an acute MI. He was hemodynamically stable. How would YOU interpret the ECG in Figure-1 ?
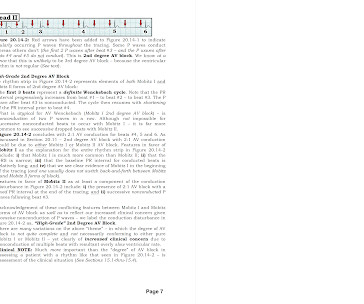
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. Section 2F ( 6 pages = the " short " Answer ) from my ECG-2014 Pocket Brain book provides quick written review of the AV Blocks ( This is a free download ). QUESTIONS: HOW would you interpret the rhythm in Figure-1 ? Is a pacemaker needed?
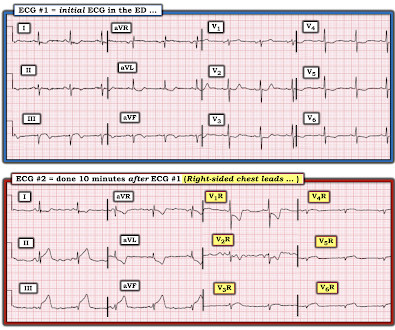
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. J of National Association of EMS Physicians 2014. E CG # 1 was obtained in the referral hospital, approximately 2 hours after the onset of chestpain. Meisel et al.
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chestpain. Figure-1: Illustration of the rational for the Mirror Test ( Figure excerpted from Grauer K: ECG-2014 Pocket Brain ePub ).
Section 2F ( 6 pages = the " short " Answer ) from my ECG-2014 Pocket Brain book provides quick written review of the AV Blocks. PEARL # 1 ( Advanced Point ): The fact that the QRS complex is narrow, with at least some P waves — and a pattern suggesting group beating — should clue us into: i ) The possibility of Wenckebach conduction! —
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
Case 2: sent by Dr. James Alva A man in his 50s with diabetes, hypertension, and hyperlipidemia presented to the ED with chestpain and shortness of breath off and on over the past three days, with associated vomiting. M y T HOUGHTS on E CG # 1 — The patient in Case #1 was a 60-something woman with acute dyspnea, but no chestpain.
There was no chestpain. Acute posterior OMI would be a prime concern for the ECG in Figure-1 — IF the patient presented with cardiac-sounding chestpain. But today's patient had no chestpain. I was worried that the ST depression and T-wave inversion in V2 and V3 might be posterior OMI.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia.
Given the history of dyspnea on exertion over a several week period ( but no mention of chestpain ) — and — the finding of deep, symmetric T wave inversion in the anterior leads ( as per Pearl #2 ) — it is possible that the onset of her symptoms is the result of a "Silent MI" ( See ECG Blog #228 for more on "Silent" MI ).
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. 10 The 2014 ACC/AHA guidelines for the Management of Patients with Valvular Heart Disease , referencing this article, gives this recommendation: "CLASS IIb 1.
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. We need more such ECGs for training but we are constantly working on the algorithm and one day it will make this diagnosis. == But isn't ongoing chestpain in NSTEMI a guideline indication for emergent angiography?
This was NOT high sensitivity troponin, but we know from a couple studies that, even using hs-cTnI, Unstable angina still exists: These two slides come from my recent lecture on high sensitivity troponin : Slide 23 in the lecture. Thelin et al.
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. History Patient complains of a 24-hours of chestpain of sudden onset, sharp in nature. Denies SOB.
A 62 year old man with hyperlipidemia presented to a rural emergency department with 7 hours of 3/10 chestpain. Figure-2: Illustration of the rational for the Mirror Test ( Figure excerpted from Grauer K: ECG-2014 Pocket Brain ePub ). =
The ECG in Figure-1 was obtained from a middle-aged man who presents to the ED ( E mergency D epartment ) with 6 hours of chestpain. Figure-1: The initial ECG in today's case obtained from a middle-aged man with 6 hours of chestpain. ( He is hemodynamically stable.
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. Note characteristic ballooning of the apex and hypercontractility of the base during cardiac cath ( Figure excerpted from Grauer K: ECG-2014- Expanded ePub, KG/EKG Press ). = Journal of Geriatric Cardiology , 19 (6). Virmani, R., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content