This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Introduction:Real-world data showed that less than half of the acute ischemic stroke (AIS) patients with large vessel occlusion (LVO) presenting with low Alberta Stroke Program Early Computed Tomography Score (ASPECTS) (2-5) achieved favorable outcomes at 90 days after mechanical thrombectomy (MT). was related to 90-day mRS 0-3.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
This can be simply a equivalent of HT, with no true supply side ischemia with LVF with global ST depression ) Management *More or less similar to STEMI with aggressive opening of culprit lesions with few differences. Outcome There are differing data about prognosis of CS in STEMI vs NSTEMI. Circ Cardiovasc Qual Outcomes.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
This ECG is diagnostic of diffuse subendocardial ischemia. Data collected included demographics, initial rhythm, EKG, emergency department (ED) CT and outcomes. The data was analyzed in relation to initial rhythm, outcomes and changes or delay in treatment. This is due to the severity of brain damage.
5 Over my career as a cardiovascular surgeon, as well as an immunologist, I have witnessed how current treatments for ASCVD have led to considerable improvements in outcomes, yet many patients remain vulnerable to life-threatening cardiac events.1,6 2013;368(21):2004-2013. Published 2013 Apr 4. 12 Colchicine, 0.5 N Engl J Med.
This suggests further severe ischemia. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. Detailed coronary artery evaluation not performed. Exam was interpreted and discussed with Dr. Simegn of cardiology, who reviewed the cardiac portion.
Outcome: Patient ruled out for MI by troponins. And ECGs can change and evolve even when there is no ischemia. Although this is not a common phenomenon — You will see it on occasion ( See the July 24, 2013 post , among others — in Dr. Smith's ECG Blog ). Here is a great case of pseudonormalization. Here are multiple cases.
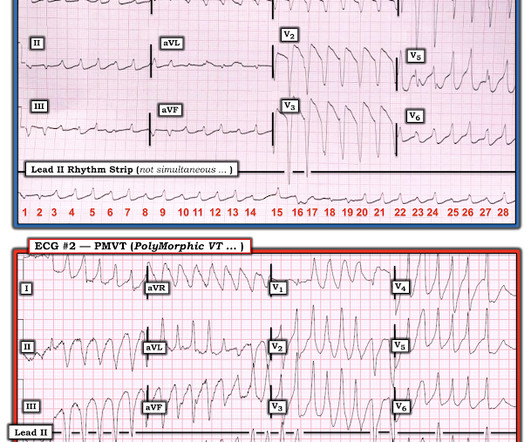
COMPARE ECG #1 with ECG #2: I think the easiest way to make the case for Pleomorphic VT is to compare the 2 tracings in Figure-3: I took ECG #2 in Figure-2, from the October 12, 2013 post in Dr. Smith’s ECG Blog. Classification of the morphologic type of VT may provide clues to etiology, outcome and treatment.
This case was texted to me by one of our residency graduates, and with the outcome, so I don't know how I would have interpreted it blindly. Chest pain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated. is worrisome!
EKG shown here: LAFB with no clear signs of OMI or ischemia. Queen of Hearts Interpretation: Would 20 minutes earlier diagnosis have made a difference in his clinical outcome? EKG and CT head were performed. Imaging was negative and he was discharged home.
1] The patient did not have a good outcome because their ECG was labeled ‘normal’ but in spite of it. Ischemic ST-segment depression maximal in V1-V4 (versus V5-V6) of any amplitude is specific for Occlusion Myocardial Infarction (versus nonocclusive ischemia). Arch Cardiovasc Dis 2013 Khan AR et al.
Objective:To investigate the treatment outcomes of MT in tVBO.Method:This international, multicenter, retrospective cohort included patients with MT for tVBO and isolated BAO from 2013 to 2023. The primary outcome was the 90-day modified Rankin Scale (mRS) score 0-2. Of those, 61 (9.7%) had a tVBO. 7.85; P=0.002).
Denying patients the potential benefit of revascularization just because their symptoms have lasted a certain amount of time shows poor understanding of the pathophysiology of myocardial ischemia. There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior. link] [2] Oliva, P.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Was her outcome to be expected for ostial RCA OMI? The patient certainly had OMI and received treatment for it. SanzRuiz, R.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content