This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology. N Engl J Med 2003; 348:1756-1763, 5/1/2013.
STE limited to aVR is due to diffuse subendocardial ischemia, but what of STE in both aVR and V1? The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Was this: 1) ACS with ischemia and spontaneous reperfusion?
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
As a result — IF no "fixable" cause is found ( ie, ischemia/infarction — electrolyte disturbance — rate-slowing medication ) — then because of the AV block and very slow heart rate, this patient will probably need a pacemaker. There are also twice as many P waves as QRS complexes — so at the least, there is 2nd-degree AV block.
This can be simply a equivalent of HT, with no true supply side ischemia with LVF with global ST depression ) Management *More or less similar to STEMI with aggressive opening of culprit lesions with few differences. 2013 Nov;6(6):708-15. Epub 2013 Nov 12. PMID: 35743628; PMCID: PMC9224589. Circ Cardiovasc Qual Outcomes.
Objective:To assess whether diffusion restriction (DR) of the retina and optic nerve (ON) can be accurately and reliably identified on standard stroke protocol brain magnetic resonance diffusion-weighted imaging (DWI-MRI) in patients presenting with acute non-arteritic central retinal artery occlusion (CRAO).Background:Retinal
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
In this study, we aim to investigate the relationship between the number of MT passes at which successful recanalization is obtained and outcomes in LVO-related AIS patients with low ASPECTS.Methods:This retrospective cohort study was performed on the data from 31 thrombectomy-capable centers between 2013 to 2022.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
Int J Cardiol 2013 2. We are told that the Stress Echo that was performed showed objective evidence of inducible ischemia ( confirmed apparently by both wall motion abnormalities and ECG changes ). Was this objective evidence of inducible ischemia accompanied by chest pain? Backus BE, Six AJ, Kelder JC, et al.
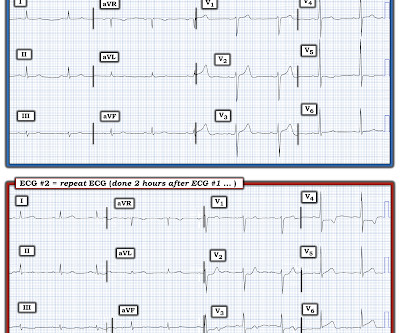
Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada. Ischemia/infarction. Acute febrile illness. Hypothermia.
This suggests further severe ischemia. There is 1 mm of ST segment elevation in lead aVR — which in the context of ST segment flattening in most other leads, suggests that there may be a component of subendocardial ischemia from underlying coronary disease. Detailed coronary artery evaluation not performed. Downstream vasospasm?
There is no ischemia, certainly no concern at all for OMI. These ER patients did not have ischemia — and the variation in ST elevation was not related to either heart rate or QRS amplitudes ( Variation in ST-Segment Elevation in Early Repolarization: Electrocardiography 40:10,2007 ).
Although this " Imbalance " of precordial T waves is not see n very often — in the “right” clinical setting, it has been associated with recent OMI ( O cclusion-based MI ) , most often from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM — and ECG Blog #350 ).
This ECG is diagnostic of diffuse subendocardial ischemia. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
mg reduced the risk of cardiovascular death, MI or heart attack, ischemic stroke, or ischemia-driven coronary revascularization by 31% compared with placebo.34 2013;368(21):2004-2013. Published 2013 Apr 4. This in turn leads to an overall reduction in IL-6 production and CRP concentration.12 12 Colchicine, 0.5 N Engl J Med.
And ECGs can change and evolve even when there is no ischemia. Although this is not a common phenomenon — You will see it on occasion ( See the July 24, 2013 post , among others — in Dr. Smith's ECG Blog ). LEARNING POINT : 1. Morphology matters. Pattern recognition is essential. AI does a great job at this but most humans do not.
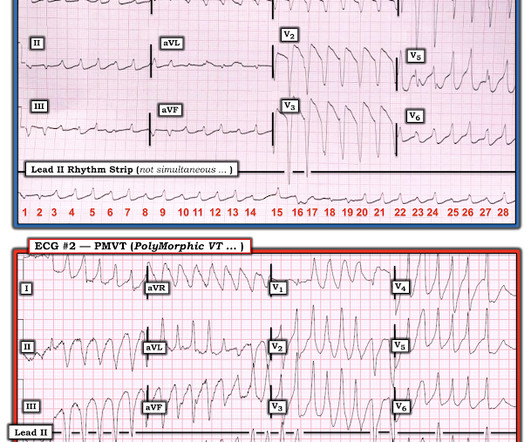
COMPARE ECG #1 with ECG #2: I think the easiest way to make the case for Pleomorphic VT is to compare the 2 tracings in Figure-3: I took ECG #2 in Figure-2, from the October 12, 2013 post in Dr. Smith’s ECG Blog. Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia.
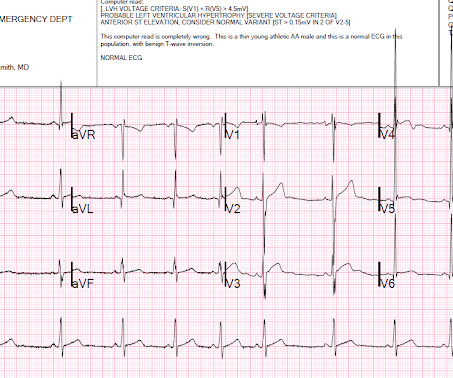
The overall ST-T wave appearance in this lead looks more like LV “strain” than ischemia. ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). T waves are upright and peaked in anterior leads V1,V2,V3.
This suggests ischemia of uncertain duration. Section 20 ( 54 pages = the " long " Answer ) from my ACLS-2013-Arrhythmias Expanded Version provides detailed discussion of WHAT th e AV Blocks are — and what they are not ! There is deep, symmetric T wave inversion with a prolonged QTc interval in anterior leads V1,V2,V3.
Chest pain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated. This was formerly an indication for cath lab activation, but was abandoned in the 2013 guidelines because of poor specificity. is worrisome!
This definition was changed following an expert consensus panel in 2013 — so that all that is currently needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern, without need for additional criteria. Panel B in Figure-1 illustrates the Brugada Type-2 or “Saddle-back” ECG pattern.
Here is his ECG: There is no clear evidence of OMI or ischemia. This " imbalance of precordial T waves" is not seen very often — and in the “right” clinical setting, has been associated with recent OMI from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM ).
EKG shown here: LAFB with no clear signs of OMI or ischemia. 8 , 9 The most recent American College of Cardiology and American Heart Association ST-elevation myocardial infarction (STEMI) guidelines (2013) give no direction on diagnosing occlusion myocardial infarction in patients with ventricular paced rhythm. No labs were performed.
2013 Sep;26(9):965-1012.e15. Alternation in ST segment appearance ( or in the amount of ST elevation or depression ) — is often linked to ischemia. J Am Soc Echocardiogr. doi: 10.1016/j.echo.2013.06.023. 2013.06.023. PMID: 23998693. Appleton C, Gillam L, Koulogiannis K. Cardiac Tamponade. Cardiol Clin. 2017 Nov;35(4):525-537.
There is no ST depression in V6, II, III, or aVF, and no significant ST elevation in aVR, all confirming that the ST vector is not consistent with diffuse subendocardial ischemia, but rather a focal ST vector pointed at the posterior wall. There is sinus rhythm with normal QRS complex and ST depression in V2-V5, maximal in V3-V4.
This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern, without need for additional criteria.
Ischemic ST-segment depression maximal in V1-V4 (versus V5-V6) of any amplitude is specific for Occlusion Myocardial Infarction (versus nonocclusive ischemia). Arch Cardiovasc Dis 2013 Khan AR et al. JAHA 2022 Grosmaitre P et al.
Below is a refresher on appropriate precordial lead placement. [6] 6] A more robust examination of lead malposition can be found at the Emergency Medicine Cases website by the great Dr. Jesse McLaren. link] Also, do not miss Dr. Grauer's great explanations on -- LAFB [link] RBBB-LBBB-IVCD [link] LBBB-Sgarbossa-LVH-MI [link] [1] Ravi, S.,
This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern, without need for additional criteria. Panel B in Figure-5 illustrates the Brugada Type-2 or “Saddle-back” ECG pattern.
Objective:To investigate the treatment outcomes of MT in tVBO.Method:This international, multicenter, retrospective cohort included patients with MT for tVBO and isolated BAO from 2013 to 2023. Secondary outcomes included complete recanalization (modified Thrombolysis in Cerebral Ischemia [mTICI] ≥ 2C) and 90-day mortality rate.
Doesn't this necessarily mean that he was having ischemia? Although this is not a common phenomenon You will see it on occasion ( See the June 30, 2023 post the November 27, 2023 post and the July 24, 2013 post in Dr. Smith's ECG Blog ). What does the Queen of Hearts think? "No Unfortunately, life is not so simple.
Denying patients the potential benefit of revascularization just because their symptoms have lasted a certain amount of time shows poor understanding of the pathophysiology of myocardial ischemia. There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior. link] [2] Oliva, P.
Section 20 ( 54 pages = the " long " Answer ) from my ACLS-2013-Arrhythmias Expanded Version provides detailed discussion of WHAT the AV Blocks are and what they are not ! ECG Blog #184 illustrates the " m agical" m irror- i mage o pposite relationship with acute ischemia between lead I II and lead a VL.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Here is the final angiogram following placement of a stent in the ostial RCA. SanzRuiz, R., Solis, J., & & FernndezAvils, F.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content