This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Other trials that evaluated this subject were the WOEST trial (2013), Pioneer AF-PCI trial (2016), and ISAR-TRIPLE (2015). ACS QID 3103 A 64 year old Caucasian male with a history of extensive tobacco use, hypertension, hyperlipidemia, and obesity presents with acute onset chestpain. Incorrect Answers: A and E. Question 2.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. He complained of generalized weakness and left lower extremity numbness. What is it?
The ECG in Figure-1 was obtained from an older woman — who presented with chestpain and palpitations over the previous hour. She had a history of hypertension, and was on medication for this — but she was otherwise healthy. BP = 140/90 mm Hg in association with the rhythm in Figure-1. How would YOU interpret the rhythm in Figure-1 ?
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ).
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. It was from a patient with chestpain: Note the obvious Brugada pattern. A rectal temperature was obtained which read 107.9 This patient ruled out for MI.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia. 2013 Sep;26(9):965-1012.e15. She was noted to be tachycardic and her heart sounds were distant on physical exam.
His comments/questions are inserted below the ECG: A 50-something woman presented with 3 days of intermittent chestpain that became worse on the day of presentation, with diaphoresis and radiation to the left arm, as well as abdominal pain. This is her ECG: An obvious STEMI, but which artery?
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Am J Cardiol 12(9):1379-1383; Nov 2013. Optimal QT interval correction formula in sinus tachycardia for identifying cardiovacular and mortality risk: Findings from the Penn Atrial Fibrillation Free study.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. N Engl J Med 2003; 348:1756-1763, 5/1/2013. This was contributed by some folks at Wake Forest: Jason Stopyra, Shannon Mumma, Sean O'Rourke, and Brian Hiestand.
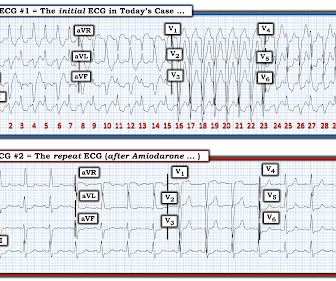
The ECG in Figure-1 was obtained from a middle-aged man who presents to the ED ( E mergency D epartment ) with 6 hours of chestpain. Figure-1: The initial ECG in today's case obtained from a middle-aged man with 6 hours of chestpain. ( He is hemodynamically stable. However, Atropine is not benign.
A middle-age woman with no previous cardiac history called 911 for chestpain. This was her prehospital ECG: What do you think? There is sinus rhythm with RBBB and obvious LAD OMI (proximal LAD occlusion): hyperacute T-waves in I, aVL and minimal STE in V1, V2. DOI: 10.1016/j.resuscitation.2025.110515
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. This was overtaken by a predominance of sympathetic surge ( tachycardia, persistent ST elevation development of electrical "storm" with failure to respond to recurrent defibrillation ). SanzRuiz, R., Solis, J., & link] Bai, J.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content