This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. And yet it still says "normal".
The patient presented with chestpain. If it is STEMI, it would have to be RBBB with STEMI. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. This ECG was sent from South Asia.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! But if there is none - then you are looking at least at an Isolated Posterior STEMI until proven otherwise.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Int J Cardiol 2013 2. Shin YS, Ahn S, Kim YJ.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Limkakeng AT.
Written by Pendell Meyers, few edits by Smith A man in his 60s with history of stroke and hypertension but no known heart disease presented with chestpain that started on the morning of presentation at around 8am. So it is very unclear to me whether or not "posterior STEMI" is actually a recognized entity under our current guidelines.
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute.
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI.
A 40-something male with no previous cardiac disease presented with chestpain. The pain continued and the first high sensitivity troponin I returned at 105 ng/L Another ECG was recorded: The ST segment in aVF has flattened a bit, revealing that there is some STD in addition to the non-specific findings in III and aVL.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This 50-something otherwise healthy male presented with one hour of epigastric and lower chestpain. One of our fine interns, Daniel Lee, who is also an ECG whiz, found this paper from 2013 and brought it to my attention: The delayed activation wave in non-ST-elevation myocardial infarction. This is hard to tell.
Steffen writes this case: "A few weeks ago I was able to recognize a STEMI because of what I had seen on your blog." "I I have enclosed the ECG from a 50-something year old male who complained of chestpain. For clarity — I’ve labeled the compressed 12-lead tracing of this 50-ish year old man with new chestpain ( Figure-1 ).
Although this " Imbalance " of precordial T waves is not see n very often — in the “right” clinical setting, it has been associated with recent OMI ( O cclusion-based MI ) , most often from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM — and ECG Blog #350 ).
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
Other trials that evaluated this subject were the WOEST trial (2013), Pioneer AF-PCI trial (2016), and ISAR-TRIPLE (2015). ACS QID 3103 A 64 year old Caucasian male with a history of extensive tobacco use, hypertension, hyperlipidemia, and obesity presents with acute onset chestpain. Incorrect Answers: A and E. Question 2.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. What is it?
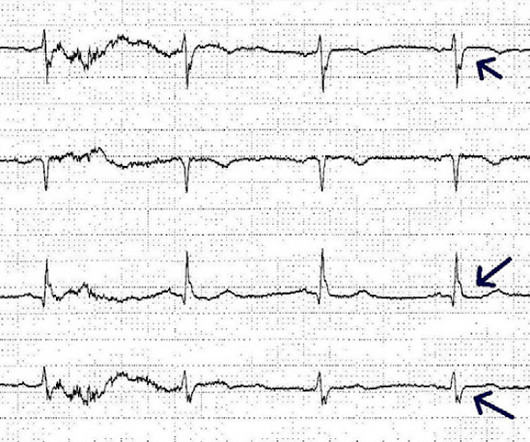
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
Although this " Imbalance " of precordial T waves is not seen very often — in the “right” clinical setting, it has been associated with recent OMI ( O cclusion-based MI ) from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM — and ECG Blog #350 ).
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. It was from a patient with chestpain: Note the obvious Brugada pattern. Bicarb 20, Lactate 4.2,
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. What do you see?
A 26 year old male presented with syncope and chestpain. Smith : I recognize this as a STEMI mimic. No signs of OMI" The chestpain resolved after some time, and another ECG was recorded: The ST Elevation is nearly gone. Syncope was sudden and without prodrome, and resulted in head trauma with a scalp laceration.
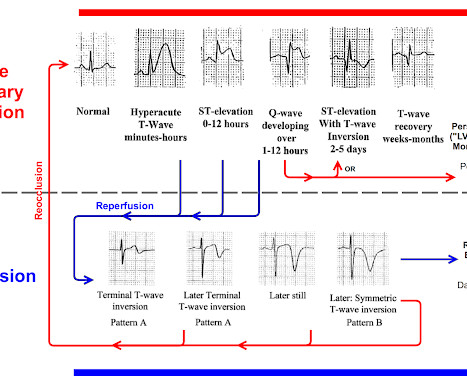
Scenario 1 : The patient presents with 24 hours of substernal chestpain. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). He presented to the emergency department for evaluation.
The ECG in Figure-1 was obtained from a middle-aged man who presents to the ED ( E mergency D epartment ) with 6 hours of chestpain. Figure-1: The initial ECG in today's case obtained from a middle-aged man with 6 hours of chestpain. ( He is hemodynamically stable.
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ). SanzRuiz, R., Solis, J., & & FernndezAvils, F. link] Bai, J.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content