This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The sooner a lay rescuer (bystander) starts cardiopulmonary resuscitation (CPR) on a person having a cardiacarrest at home or in public, up to 10 minutes after the arrest, the better the chances of survival and brain protection, according to an analysis of nearly 200,000 out-of-hospital cardiacarrest cases in the U.S.
Weekend procedures also face limited access to specialized cardiac teams, affecting timely decisions and making urgent procedures more difficult to schedule. Beyond in-hospital mortality, weekend patients faced a 3.27x higher risk of death following the procedures.
Background:Prompt initiation of bystander cardiopulmonary resuscitation (CPR) is critical to survival for out-of-hospital cardiacarrest (OHCA). Results:Of 78 048 patients with a witnessed OHCA treated with bystander CPR, the mean age was 63.5±15.7 years and 25, 197 (32.3%) were women.
What is the utility of a head CT in cardiacarrest? We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. in Vienna found that 27 of 765 (4%) of out of hospital cardiacarrests (OHCA) were due to SAH.
BackgroundTelecommunicator CPR (T‐CPR), whereby emergency dispatch facilitates cardiacarrest recognition and coaches CPR over the telephone, is an important strategy to increase early recognition and bystander CPR in adult out‐of‐hospital cardiacarrest (OHCA). Journal of the American Heart Association, Ahead of Print.
Cardiacarrest can cause diffuse subendocardial ischemia, usually transient (it often resolves as time goes by after ROSC). Also, anterior MI could result from 1) ACS, but also from 2) severe ischemia due to combination of a hemodynamically significant LAD stenosis + severe hypotension during cardiacarrest.
Shortly after arrival in the ED ( E mergency D epartment ) — she suffered a cardiacarrest. BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Figure-1: The initial ECG in today's case — obtained after successful resuscitation from cardiacarrest. ( No CP ( C hest P ain ).
Steve, what do you think of this ECG in this CardiacArrest Patient?" A woman in her 50s with dyspnea and bradycardia A patient with cardiacarrest, ROSC, and right bundle branch block (RBBB). HyperKalemia with CardiacArrest. Is this just right bundle branch block?
mg experienced a 23% lower incidence of death from cardiovascular causes, resuscitated cardiacarrest, myocardial infarction, stroke, or urgent hospitalization for angina leading to coronary revascularization in a time-to-event analysis. 2013;368(21):2004-2013. Published 2013 Apr 4. 12 Importantly, colchicine, 0.5
Unfortunately, before this could be accomplished — the patient went into cardiacarrest. She was successfully resuscitated — with a post-arrest rhythm similar to that seen in Figure-1. Cardiac cath did not reveal significant coronary disease!
ST elevation (STE) in lead augmented vector right (aVR), coexistent with multilead ST depression, was endorsed as a sign of acute occlusion of the left main or proximal left anterior descending coronary artery in the 2013 STEMI guidelines. Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography.
This definition was changed following an expert consensus panel in 2013 — so that all that is currently needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern, without need for additional criteria. Panel B in Figure-1 illustrates the Brugada Type-2 or “Saddle-back” ECG pattern.
This ECG pattern may be diagnostic of B rugada S yndrome IF seen in association with: i ) a history of cardiacarrest; polymorphic VT; or of non-vagal syncope; and / or ii ) a positive family history of sudden death at an early age; and / or iii ) a similar ECG in relatives. This is not RBBB ( TOP LEFT in Figure-2 ).
In addition to a spontaneous or induced Brugada-1 ECG pattern, criteria for B rugada S yndrome require one or more of the following: History of cardiacarrest, of polymorphoic VT, or of non-vagal syncope — positive family history of sudden death at an early age — a similar ECG in close relatives.
2013 Sep;26(9):965-1012.e15. Cardiac Tamponade. American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2013.06.023.
BackgroundOut‐of‐hospital cardiacarrest survival rates have improved over time. Sex differences in temporal trends were evaluated with age‐adjusted Poisson regression analysis, including interaction for sex and out‐of‐hospital cardiacarrest year. 1.05]), with a stronger difference after 2013. in men and 15.7%
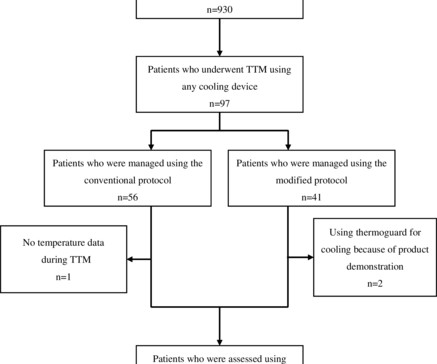
The target temperature tended to be modified worldwide after the TTM trial in 2013. Methods This single-centre, retrospective, observational study included adult out-of-hospital cardiacarrest patients who underwent TTM between April 2013 and October 2019.
BackgroundBystander cardiopulmonary resuscitation (B‐CPR) and defibrillation for out‐of‐hospital cardiacarrest (OHCA) vary by sex, with women being less likely to receive these interventions in public. CARES collected 457 621 arrests (2013–2019); after appropriate exclusion, 309 662 were included.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content