This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
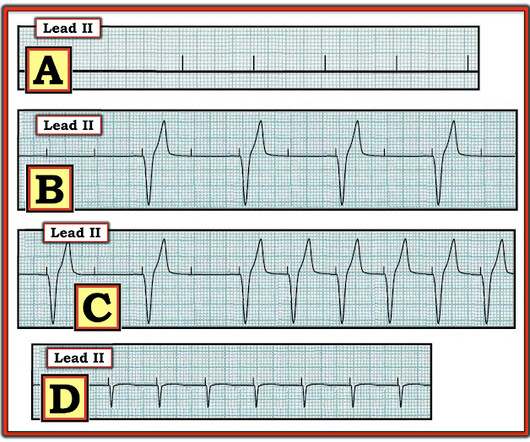
Is a pacemaker needed? Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. The patient may need a pacemaker. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. =
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study. be regular! —
Several days into hospitalization, she continued to have occasional episodes of sinus rhythm and sinus bradycardia with periods of Mobitz I AV block and 2:1 block. Meanwhile, the patient's native rhythm is sinus bradycardia with adequate perfusion. adapted from Grauer K: ACLS-2013-ePub Section 15, KG/EKG Press ).
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. 2:34 PM, following right heart catheterization She then went into atrial fibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content