This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Even if we stopped here — We could conclude the following: There is marked bradycardia in today's rhythm ( ie, Heart rate in the low 30s ). Finally — If today's patient does not have significant underlying coronary disease — then her bradycardia with AV block may be the result of SSS ( S ick S inus S yndrome ).
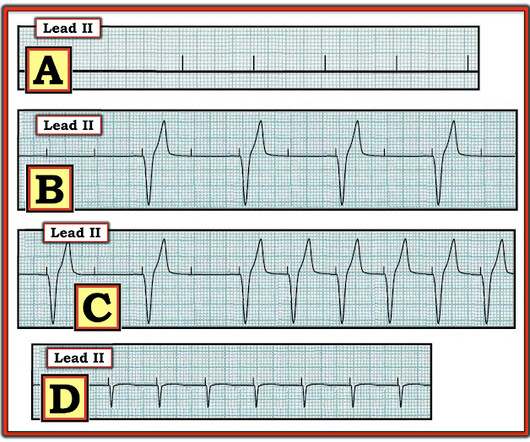
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. = Would you approve her for a nonemergent surgical procedure?
The purpose of this case series is to provide an overview of the procedural and clinical outcomes of patients who underwent stenting for symptomatic ICAS.MethodsWe reviewed a database of all interventional procedures conducted at our institution to identify patients who underwent intracranial stenting from 2013 and 2022 for symptomatic ICAS.
That said — obvious findings include: i ) Marked bradycardia! — Section 20 ( 54 pages = the " long " Answer ) from my ACLS-2013-Arrhythmias Expanded Version provides detailed discussion of WHAT th e AV Blocks are — and what they are not ! The rhythm in Figure-1 is complex — and defies precise interpretation without careful study.
Hyperkalemia causes peaked T waves and the "killer B's of hyperkalemia", including bradycardia, broad QRS complexes, blocks of the AV node and bundle branches, Brugada morphology, and otherwise bizarre morphology including sine wave. With a twist. Do you recognize this ECG yet? Right Bundle Branch Block with ST Elevation in V1?
Bradycardia. This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern, without need for additional criteria. Acute febrile illness. Variations in autonomic tone. Hypothermia.
The Initial ECG in Today's Case: ECG #1 showed sinus bradycardia at a rate slightly under 60/minute — normal intervals — slight left axis ( about -15 degrees ) — and no chamber enlargement. Figure-1: I've labeled the 1st, 2nd and 4th tracings in today's case ( See text ).
Whatever today's rhythm turns out to be — the "good news" is that the bradycardia and degree of AV block is likely to improve as soon as there is reperfusion of the "culprit" artery ( Therefore need for prompt cath with PCI ).
This definition was changed following an expert consensus panel in 2013 — so that at the present time, all that is needed to diagnose Brugada Syndrome is a spontaneous or induced Brugada-1 ECG pattern, without need for additional criteria.
Several days into hospitalization, she continued to have occasional episodes of sinus rhythm and sinus bradycardia with periods of Mobitz I AV block and 2:1 block. Meanwhile, the patient's native rhythm is sinus bradycardia with adequate perfusion. adapted from Grauer K: ACLS-2013-ePub Section 15, KG/EKG Press ).
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ). He told the patient this horrible news. SanzRuiz, R.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content