This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
88% of patients in the Tailored cohort experienced freedom from AF 12 months after one procedure with or without anti-arrhythmic drugs compared to 70% in the Anatomical cohort (log rank p In the Tailored cohort, patients experienced a higher rate of freedom from any arrhythmia after 1.2 Am J Cardiol 2013; 112:11421147.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:Epicardial radiofrequency catheter ablation (RFCA) of idiopathic ventricular arrhythmias (VAs) originating from the left ventricular summit (LVS) is challenging because of the anatomic barriers.
The Zio monitor ECG System secured its CE mark based on compliance to EU MDR standards of performance, quality, safety, and efficacy, along with the body of clinical evidence supporting Zio in detecting potential cardiac arrhythmias. Diagnostic Utility of a Novel Leadless Arrhythmia Monitoring Device, American Journal of Cardiology , 2013.
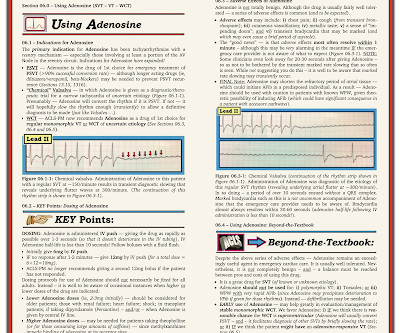
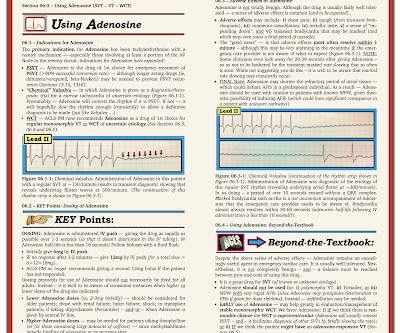
MY Thoughts on the ECG in Figure-1: When faced with a challenging cardiac arrhythmia — It is a "luxury" to have access to a long lead rhythm strip containing 3 simultaneously -recorded leads. Figure-5: Pages 1 and 2 on Pros & Cons of using Adenosine ( excerpted from my ACLS-2013-ePub ). QUESTIONS: Is the rhythm AVNRT or AVRT?
With P waves labeled — Isn't it now much easier to appreciate that the atrial rhythm is quite regular ( with no more than a slight sinus arrhythmia )? P utting I t A ll T ogether : The precise mechanism of today's arrhythmia is complex and difficult to determine. For those with a special interest in cardiac arrhythmias — READ ON! —
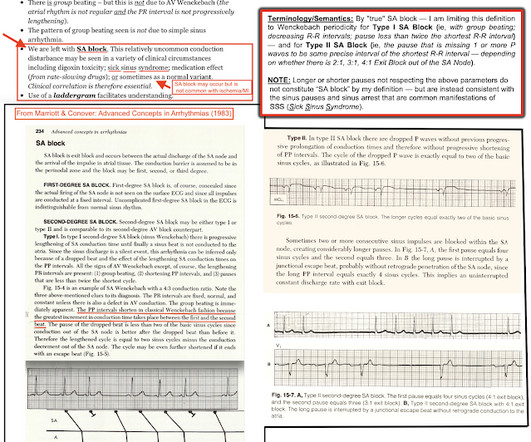
Because of underlying sinus arrhythmia — the P wave in front of beat #6 occurs at an opportune time, and is able to conduct to the ventricles. Section 20 ( 54 pages = the " long " Answer ) from my ACLS-2013-Arrhythmias Expanded Version provides detailed discussion of WHAT the AV Blocks ar e — and what they are not !
NOTE: There may be slight variation in the P-P interval if some sinus arrhythmia is present — but even then, it will usually be obvious IF the "theme" of the P-P interval is that of an underlying sinus rhythm. This highlights the pros and cons for using Adenosine — which I review in Figure-5 and Figure-6 ( excerpted from my ACLS-2013-ePub ).
Volta Medical has announced it has entered into a Joint Development Agreement with GE Healthcare to enhance arrhythmia procedures with artificial intelligence (AI)-driven electrophysiology technologies. Am J Cardiol 2013; 112:1142–1147. 1 Approximately 33 million patients worldwide are living with AFib. adult population.
Section 20 ( 54 pages = the " long " Answer ) from my ACLS-2013-Arrhythmias Expanded Version provides detailed discussion of WHAT the AV Blocks are — and what they are not ! Section 2F ( 6 pages = the " short " Answer ) from my ECG-2014 Pocket Brain book provides quick written review of the AV Blocks ( This is a free download ).
[link] == MY Comment , by K EN G RAUER, MD ( 8/5 /2024 ): == As one who has been fascinated by cardiac arrhythmias for decades — I find the most difficult aspect of rhythm interpretation for me, is distinguishing between what is "real" vs what is artifact, or simply background "noise". We learn best when we learn from each other.
Whatever the specific etiology of today's arrhythmia is, the “good news” is — that this rhythm will most probably improve with reperfusion of the "culprit" artery. That said — I found today's arrhythmia fascinating, and worthy of more in-depth analysis. Using calipers facilitates the process.
This familial cardiac arrhythmia is the result of gene mutation. These patients are at high risk for malignant arrhythmias. Typically — these arrhythmias are induced by exercise or intense emotional states ( ie, associated with increased catecholamine discharge ). The heart is structurally normal in patients with CPVT.
Realizing that slight variation in the P-P interval is common ( known as sinus arrhythmia ) — the PINK arrows in Figure-3 suggest the probable location of underlying sinus P waves. Certain complex arrhythmias may have more than a single plausible rhythm interpretation. This is precisely what we see in Figure-4.
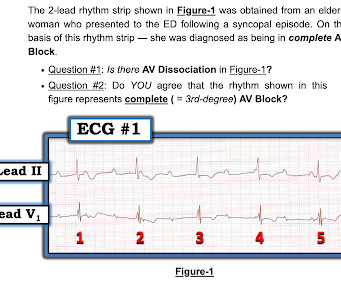
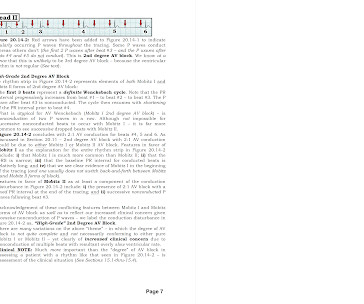
KEY Point: When most beats in an arrhythmia are regular, but some are not — the best CLUE to interpretation often resides in looking for a “ break ” in the rhythm ( such as is seen between beats #13 and 14 in Figure-2 ). The simple step of labeling all of the obvious P waves — is surprisingly helpful in evaluating the rhythm.
Section 20 ( 54 pages = the " long " Answer ) from my ACLS-2013-Arrhythmias Expanded Version provides detailed discussion of WHAT th e AV Blocks are — and what they are not ! — — E CG M edia P EARL # 75 ( 6:10 minutes Audio ) — Reviews how to tell IF a J unctional ( AV Nodal ) R hythm is p athologic or a ppropriate ?
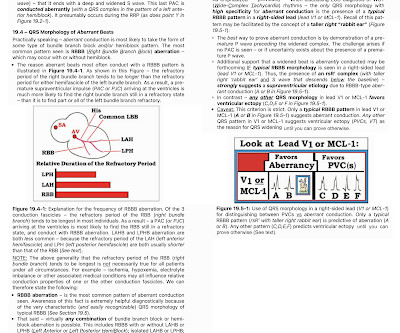
. == PEARL # 2: As discussed in ECG Blog #389 — the saying, "Birds of a Feather Flock Together" — serves as a helpful reminder of an important concept in arrhythmia interpretation. A DDENDUM ( 8/19/2023 ) In the following 3 Figures — I post written summary from my ACLS-2013-ePub regarding the basics of Aberrant Conduction.
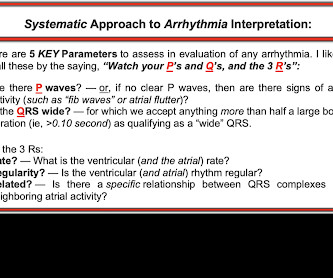
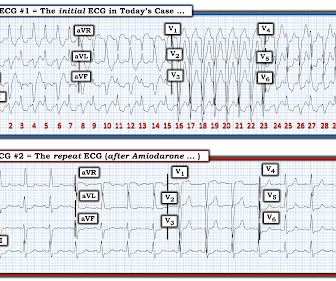
What is unusual about this arrhythmia? Doing so suggests that the R-R interval of this exceedingly rapid arrhythmia is just a tiny amount over 1 large box — which corresponds to a ventricular rate just under 300/minute ( ie, between 290-300/minute ). How would YOU interpret the ECG in Figure-1 ?
Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. In light of the risk of arrhythmia events observed in the Mizusawa trial, a formal EP study might be reasonable to obtain in those with fever induced asymptomatic Brugada ECG changes to help risk stratify these patients.
Arrhythmias : A leadless pacemaker-defibrillator system provides antitachycardia pacing for ventricular tachycardia in patients with subcutaneous ICDs. Preventive Cardiology : The new PREVENT risk calculator is more accurate than the 2013 PCEs’ ASCVD risk estimates and is recommended for risk stratification.
L addergram I llustration : At this point — I needed to work out, and then draw a laddergram that I could then verify to ensure a plausible mechanism for today's arrhythmia. Note also that the P-P interval between successive P waves ( vertical RED lines ) is similar, albeit not quite equal ( ie, There is slight sinus arrhythmia ).
Having worked through the Ps,Qs,3R Approach — we have established that the QRS is wide — there is a fairly regular P wave rhythm ( albeit with slight sinus arrhythmia ) — and the ventricuar rhythm is fairly ( albeit not completely ) regular. M ore P EARLS : Determing IF there is AV Block?
PEARL # 7: As is evident for many of the examples of AV block that have appeared in this ECG Blog — it is common to see a " ventriculophasic " sinus arrhythmia in association with 2nd or 3rd degree AV block. This is a free download ).
Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. In light of the risk of arrhythmia events observed in the Mizusawa trial, a formal EP study might be reasonable to obtain in those with fever induced asymptomatic Brugada ECG changes to help risk stratify these patients.
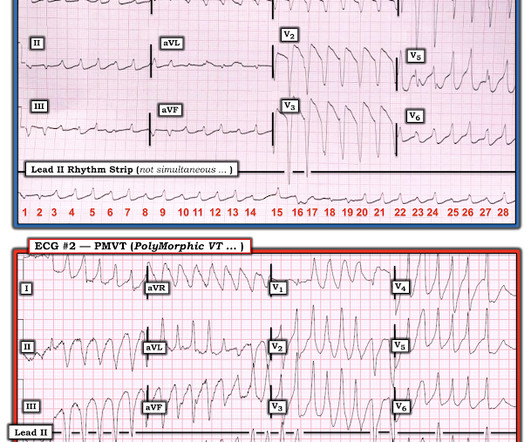
COMPARE ECG #1 with ECG #2: I think the easiest way to make the case for Pleomorphic VT is to compare the 2 tracings in Figure-3: I took ECG #2 in Figure-2, from the October 12, 2013 post in Dr. Smith’s ECG Blog. WHY CARE about QRS Morphology with VT?
But eliciting both a personal and family History on such patients ( inquiring about syncope-presyncope, or malignant arrhythmia symptoms ) — is essential for optimal management. Meyers to emphasize the strong likelihood of a benign prognosis associated with tracings like ECG #1 in Figure-1.
Finally — a detailed family history ( for early sudden death ) + a careful personal history ( for syncope/presyncope; malignant arrhythmia ) is in order.
ST elevation (STE) in lead augmented vector right (aVR), coexistent with multilead ST depression, was endorsed as a sign of acute occlusion of the left main or proximal left anterior descending coronary artery in the 2013 STEMI guidelines.
myocardial infarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. N Engl J Med 2003; 348:1756-1763, 5/1/2013. Fundamentally, cardiogenic shock is an issue of decreased cardiac output. This may be secondary to multiple factors, including decreased cardiac contractility (ie. Circulation 1970;41:623-627 9.
2013 Sep;26(9):965-1012.e15. Both ST segment and T wave alternans have been known to precede malignant ventricular arrhythmias. J Am Soc Echocardiogr. doi: 10.1016/j.echo.2013.06.023. 2013.06.023. PMID: 23998693. Appleton C, Gillam L, Koulogiannis K. Cardiac Tamponade. Cardiol Clin. 2017 Nov;35(4):525-537. doi: 10.1016/j.ccl.2017.07.006.
Overnight telemetry showed no arrhythmias ( important to reduce the risk of worrisome arrhythmia given this patient's chief complaint of sudden syncope without prodrome ). Troponins were negative. Formal contrast Echo showed normal LV function without wall motion abnormality.
MY Thoughts on Figure-1: As always I favor the P s , Q s , 3 R Approach as an optimally time-efficient way to assess any arrhythmia, including the AV blocks ( See ECG Blog #185 ). Although there is slight variation in the P-P interval this type of ventriculophasic sinus arrhythmia is common with 2nd- and 3rd-degree AV blocks.
If breakthrough ventricular arrhythmias occurred, additional 50-mg boluses were given every 5 minutes, as needed to a maximum of 325 mg. Add to this the sobering clinical reality of how difficult it is to get objective, controlled, prospective data in the emergency situation of cardiac arrest and life-threatening arrhythmias.
Section 20 ( 54 pages = the " long " Answer ) from my ACLS-2013-Arrhythmias Expanded Version provides detailed discussion of WHAT the AV Blocks are and what they are not ! Section 2F ( 6 pages = the " short " Answer ) from my ECG-2014 Pocket Brain book provides quick written review of the AV Blocks ( This is a free download ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content