This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Int J Cardiol 2013 2. Backus BE, Six AJ, Kelder JC, et al.
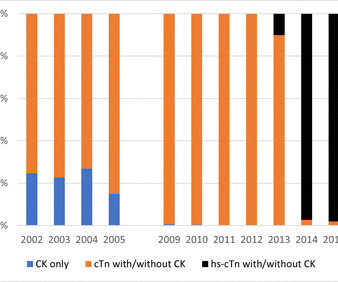
Using person-linked hospitalisation data, we compared International Classification of Diseases (ICD)-coded data with biomarker-classified admission rates for ST-segment elevation MI (STEMI), non-STEMI (NSTEMI) and unstable angina (UA) in Western Australia (WA). Results There were 37 272 ACS admissions in 30 683 patients (64.2%
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). This correlates with potentially salvageable myocardium. See Raitt et al.: These findings together are more commonly seen with pericarditis. Hammill, S.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content