This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
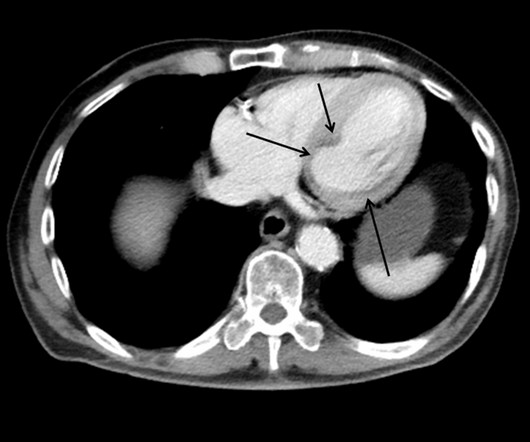
This case shows a CT image of subendocardial ischemia. However, there are also Q-waves inferiorly and the inferior T-waves are inverted, suggesting that this is an old MI with persistent ST elevation, or, alternatively, a subacute or partially reperfused, inferior STEMI. This is all but diagnostic of inferior-posterior STEMI.
He interprets here: "This EKG is diagnostic of right bundle branch block and transmural ischemia of the anterior wall, most likely from an occlusion of the proximal LAD. Pendell Meyers had not started medical school by summer of 2012, but he had read every one of my blog posts over the preceding 4 years. He was a paramedic at the time.
There may be ischemia present, but it is not evident on the ECG. LVH and the diagnosis of STEMI - how should we apply the current guidelines? This one mimics inferior STEMI (Figure 4): Concentric LVH, NO wall motion abnormality Case 5. How about diagnosing anterior STEMI in the setting of LVH? All troponins were negative.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. 109 (20):361-368, 2012 — CLICK HERE ). Which artery? Could this be myopericarditis?
If it is STEMI, it would have to be RBBB with STEMI. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). Annals of Emergency Medicine 2012; 60(12):766-776. Limkakeng AT.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. BOTTOM Line: It can at times be extremely challenging to distinguish between anterior ST elevation from a benign Brugada Phenocopy pattern vs an acute anteroseptal STEMI.
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center. It’s important to stress the presence of a normal QRS (i.e., References 1] Smith, S.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content