This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
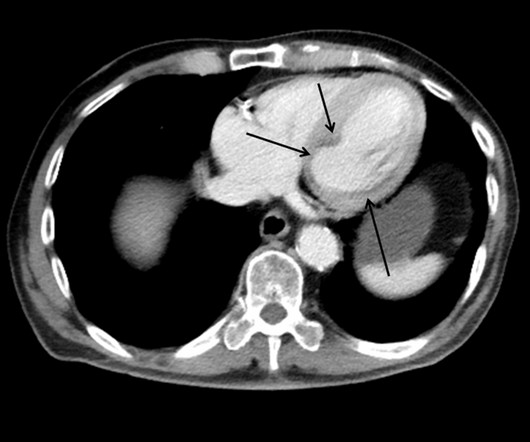
This case shows a CT image of subendocardial ischemia. The post cath ECG was not recorded until the next morning: The ischemia is almost entirely resolved. The inferior and posterior walls are also at chronic risk of subendocardial ischemia because of this tenuous blood supply. No evidence for watershed ischemia.
He interprets here: "This EKG is diagnostic of right bundle branch block and transmural ischemia of the anterior wall, most likely from an occlusion of the proximal LAD. Pendell Meyers had not started medical school by summer of 2012, but he had read every one of my blog posts over the preceding 4 years. He was a paramedic at the time.
There may be ischemia present, but it is not evident on the ECG. In this paper, Dr. Birnbaum writes: "In patients with ACS without LVH, ST depression with negative T waves in the lateral leads is a sign of sub-endocardial ischemia and is an independent predictor of adverse outcome [11 – 13]. ST elevation in V2 is about 3.5
The ECG does not show any definite signs of ischemia. Uncontrolled coronary spasm may be associated with serious arrhythmias , including cardiac arrest ( Looi et al — Postgrad Med, 2012 ; Tan et al — Eur Heart J Case Rep, 2018 ; Chevalier et al — JACC, 1998 ; Rodriguez-Manero — EP Europace, 2018 ). He denied any exertional chest pain.
Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. The ECG does not show any signs of ischemia. True Positive ECG#2 : Also sinus rhythm. There is ST depression in V1.
Mechanism is thought to be due to sustained sympathetic stimulation, probably caused by dysfunction of insular cortex resulting in reversible neurogenic damage to the myocardium which could include contraction bands and subendocardial ischemia [2]. 2012 Dec;7(4):290-4. 2012 Dec;7(4):290-4. Maedica (Bucur). Maedica (Bucur).
This study compared outcomes for patients with DOAC treatment failure who changed or retained their prestroke DOAC.Methods and ResultsThis retrospective cohort study analyzed data from the National Health Insurance Research Database from 2012 to 2020.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. 109 (20):361-368, 2012 — CLICK HERE ). She was taken to the cath lab and her coronaries were clean!! There was no MRI, but the presumptive diagnosis is myocarditis. I have seen this pattern in severe acute AI also."
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. Arbab-Zadeh, Heart Int 2012.
Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada. Ischemia/infarction. Electrocardiol 45:433-442, 2012 ).
mEq/L for Mg++ ) — given that ECF levels of these cations comprise only ~1-2% of total body stores ( Jahnen-Dechent and Ketteler — Clin Kidney J 5(Suppl 1):i3-i14, 2012 — and — Udensi and Tchounwou — Int J Clin Exp Physiol 4(3): 111-122, 2017 ). mEq/L for K+ and 1.76
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG. Also: As we always say, do not give morphine until you are committed to the cath lab. Tikkanen, J. Wellens, H., & & Yan, G.-X. link] McGee, S.
However, its refined version LMWH, though made it more palatable & user friendly, it un-apologetically took the sting out of regular heparin, made it less efficacious (more glamorous though) LMWH usage is in CAD widespread , it has suspect value* in true ongoing ischemia in any active ACS situation. 2012 May-Jun;54(3):207-15.
It’s important to stress the presence of a normal QRS (i.e., When the differential is LAD occlusion versus Normal Variant, use the formula as an assistive tool – only exercise extreme caution when reclassifying what you believe to be LAD occlusion as Normal Variant. With deliberate practice, spot diagnosis of T-to-R ratio will come with time.
These include ( among others ) — acute febrile illness — variations in autonomic tone ( as may occur with syncope ) — hypothermia — ischemia or infarction — cardiac arrest — and electrolyte disorders ( especially hyperkalemia — but also hypokalemia/hyponatremia ). Circulation, 117, 1890–1893. [3]: World Journal of Cardiology, 4(3): 84-86. [4]:
Annals of Emergency Medicine 2012; 60(12):766-776. EKG shown here: LAFB with no clear signs of OMI or ischemia. Diagnosis of Acute Myocardial Infarction in the Presence of Left Bundle Branch Block using the ST Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. No labs were performed. EKG and CT head were performed.
Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Circulation, 117, 1890–1893. [3]: 3]: Lamelas P, Labadet C, Spernanzoni F, Lopez Saubidet C, and Alvarez PA. Brugada electrocardiographic pattern induced by fever. World Journal of Cardiology, 4(3): 84-86. [4]: 4]: Antzelevitch C and Brugada R.
IF the Patient is Younger and Athletic: The mechanism of AFib in younger, athletic individuals is often heavily influenced by increased vagal tone ( Rao and Shipon — ACC, 2019 — and — Calvo et al — Br J Sports Med, 2012 ). To EMPHASIZE: The diagnosis of SSS requires ruling out other cause of inappropriately slow AFib i n the older patient.
Occurrence of “J Waves” in 12-Lead ECG as a Marker of Acute Ischemia and Their Cellular Basis. Europace 2012 Shinde R, Shinde S, Makhale C, Grant P, Sathe S, Durairaj M, Lokhandwala Y, Di Diego J, Antzelevitch C. Occurrence of "J waves" in 12-lead ECG as a marker of acute ischemia and their cellular basis.
There is ST elevation in 9/12 leads with ST depression only seen in lead aVR>V1 ( ie, virtually the opposite of what is seen with diffuse subendocardial ischemia in which there is diffuse ST depression except for ST elevation in aVR>V1 ).
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Here is the final angiogram following placement of a stent in the ostial RCA. link] Mostofsky, E., Maclure, M., Sherwood, J.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content