This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In that study commonest ECG abnormalites were QTc prolongation followed by brady/tachycardia and then ST segment deviations [3]. Cerebrovascular damage can cause cardiac arrhythmias related to disinhibition of right insular cortex with resulting increased sympathetic tone. 2012 Dec;7(4):290-4. 2012 Dec;7(4):290-4.
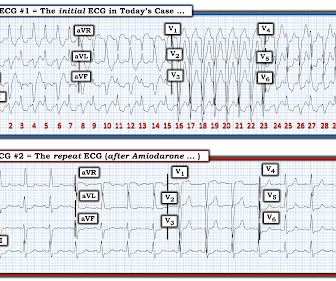
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
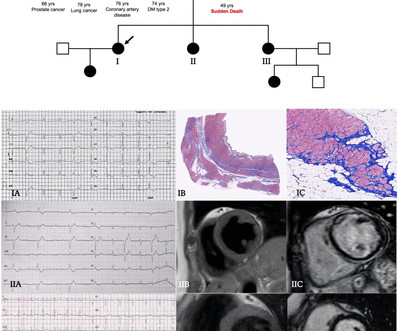
This familial cardiac arrhythmia is the result of gene mutation. These patients are at high risk for malignant arrhythmias. Typically — these arrhythmias are induced by exercise or intense emotional states ( ie, associated with increased catecholamine discharge ). The heart is structurally normal in patients with CPVT.
What is unusual about this arrhythmia? Doing so suggests that the R-R interval of this exceedingly rapid arrhythmia is just a tiny amount over 1 large box — which corresponds to a ventricular rate just under 300/minute ( ie, between 290-300/minute ). How would YOU interpret the ECG in Figure-1 ?
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
There are a number of things to look for in an ECG that can hint at arrhythmia as the cause of an apparent seizure. There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). Below are some of the conditions to be aware of: Preexcitation Brugada syndrome.
Methods Patients were retrospectively evaluated between January 2012 and June 2020. Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chest pain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%). Significant right ventricular involvement was an exclusion criterion.
I completely agree with Dr. Nossen that in this patient with new CP and sinus tachycardia with LAHB — that the T waves in each of the inferior leads are hyperacute ( ie, clearly disproportionately "bulky" given size of the QRS in these leads ). — and which other patient(s) need to be seen as soon as possible to figure out what is going on?
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. There was a 0.9% Circulation, 117, 1890–1893. [3]:
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. J Electrocardiology 45 (2012):433-442. Her temperature was 106 degrees.
While traditionally described as “benign early repolarization”, they have been associated with J wave syndromes along with Brugada syndrome, causing ventricular arrhythmias (1, 2). The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy. Indian Pacing Electrophysiol J 2004 Antzelevitch C, Yan G.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content