This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Whenever a patient does not have chestpain, the pre-test probability of OMI is diminished. Of course SOB, jaw pain, shoulder pain, etc can be a result of OMI, but the pretest probability is less and so you must scrutinize further. Lethal arrhythmias may be a terminal event ( VT/VFib; Asystole ).
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
The ECG in Figure-1 was obtained from an older woman — who presented with chestpain and palpitations over the previous hour. This familial cardiac arrhythmia is the result of gene mutation. These patients are at high risk for malignant arrhythmias. BP = 140/90 mm Hg in association with the rhythm in Figure-1.
She did notice something slightly wrong subjectively, but had no palpitations, chestpain, or SOB, or any other symptom. The Role of Sinus Arrhythmia: I found it interesting to compare the long lead II rhythm strips in the 3 serial tracings from today’s case ( Figure-1 ). She was on no medications. Potassium was normal.
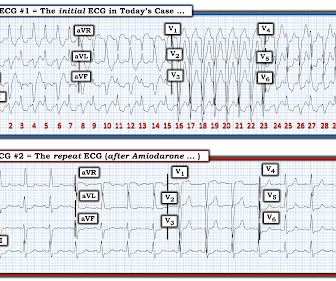
Diagnosis : Atrial flutter with 1:1 conduction, with fast AV conduction made possible by sympathetic drive of exercise On arrival, we obtained another 12-lead: Unremarkable Further history: One month history of shortness of breath on exertion, denies palpitations, chestpain, orthopnea, leg swelling.
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardial infarction of any kind. Is it Brugada pattern?
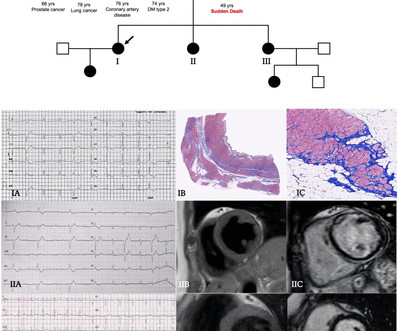
Methods Patients were retrospectively evaluated between January 2012 and June 2020. Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chestpain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%).
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7].
All of the patients presented with chestpain , and they are all in triage. Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECG s that has not been overread by a physician. Which, if any, of these patients has OMI, with myocardium at risk and need for emergent PCI?
She denied chestpain and denied feeling any palpitations, even during her triage ECG: What do you think? Free full text: [link] There are 6 categories of criteria : 1) Imaging 2) Pathologic 3) ECG Repolarization 4) ECG Depolarization 5) Arrhythmias 6) Family History. J Electrocardiol, 42 (2009), pp.
It was from a patient with chestpain: Note the obvious Brugada pattern. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. There is no further workup at this time.
J Electrocardiology 45 (2012):433-442. The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. Conclusion of this paper: Fever is a great risk factor for arrhythmia events in Brugada Syndrome patients. Bayes de Luna, A et al. Is this Type 2 Brugada syndrome/ECG pattern?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content