This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
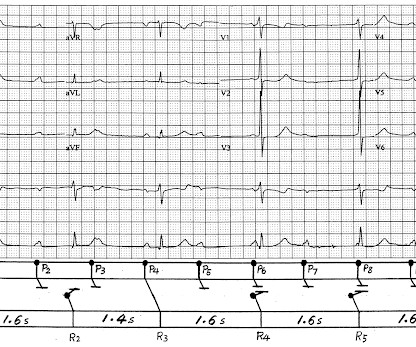
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). Initial high sensitivity troponin I returned at 6ng/L (normal 0.20
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:Epicardial radiofrequency catheter ablation (RFCA) of idiopathic ventricular arrhythmias (VAs) originating from the left ventricular summit (LVS) is challenging because of the anatomic barriers.
Cerebrovascular damage can cause cardiac arrhythmias related to disinhibition of right insular cortex with resulting increased sympathetic tone. 2012 Dec;7(4):290-4. 2012 Dec;7(4):290-4. In that study commonest ECG abnormalites were QTc prolongation followed by brady/tachycardia and then ST segment deviations [3].
This familial cardiac arrhythmia is the result of gene mutation. These patients are at high risk for malignant arrhythmias. Typically — these arrhythmias are induced by exercise or intense emotional states ( ie, associated with increased catecholamine discharge ). The heart is structurally normal in patients with CPVT.
Archives of cardiovascular diseases 105 4 (2012): 226-38.) It is gratifying that, with this study, we could sustain some confusion, in the management of this most common cardiac arrhythmia. Now, what shall we do? , Let us do another meta-analysis. A fresh one is released just a few days ago in 2024.
Between 2010 and 2012, participants completed a questionnaire, underwent a physical examination, and provided a fasting blood sample. We aimed to assess this.MethodsThis was a longitudinal analysis of data from the British Regional Heart Study, a prospective cohort study.
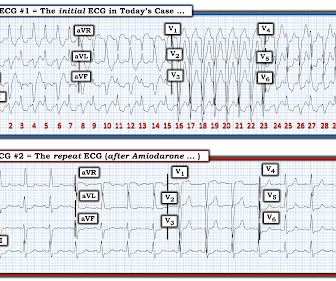
Excessive Flecainide may result in the following ( Levis — Permanente Journal 16(4): 53, 2012 ) ( Strangio et al — Eur Heart J, 2022 ) ( Andrikopoulos et al — World J Cardiol, 2015 ) ( Dardas and Khan — Eur Soc Cardiol, 2021 ) : Depressed contractility; hypotension ( negative inotropic effect ). Figure-1: The initial ECG in today's case.
IF the Patient is Younger and Athletic: The mechanism of AFib in younger, athletic individuals is often heavily influenced by increased vagal tone ( Rao and Shipon — ACC, 2019 — and — Calvo et al — Br J Sports Med, 2012 ). Note fairly marked irregularity of the R-R interval — indicative of definite sinus arrhythmia. 25, 2022 ).
What is unusual about this arrhythmia? Doing so suggests that the R-R interval of this exceedingly rapid arrhythmia is just a tiny amount over 1 large box — which corresponds to a ventricular rate just under 300/minute ( ie, between 290-300/minute ). How would YOU interpret the ECG in Figure-1 ?
A good example of the same situation was posted at “theheart.org” arrhythmia/EP section “ECG of the month” program in 2/2012. Sometimes these secondary manifestations make the tracing look more complicated and eye-catching.
IF the patient is an adult of a certain age, who has underlying heart disease — then a high level of exercise becomes increasingly likely to precipitate non-sinus tachyarrhythmias, including potential to induce malignant ventricular arrhythmias. The KEY to determine is therefore — Does the patient have underlying heart disease?
PEARL # 7: As is evident for many of the examples of AV block that have appeared in this ECG Blog — it is common to see a " ventriculophasic " sinus arrhythmia in association with 2nd or 3rd degree AV block. This is a free download ).
Though sinus bradycardia is usual, other abnormalities like sinus arrhythmia, sinus arrest, wandering atrial pacemaker and coronary sinus rhythm have been described. 2012 Jun;98(12):947-55. Athlete’s bradycardia due to increased parasympathetic tone and decreased sympathetic tone is a well-known observation. References 1.Prior
There are a number of things to look for in an ECG that can hint at arrhythmia as the cause of an apparent seizure. In my experience, the pathologic finding in the above ECG is the easiest one to overlook — especially if you are in a rush and do not do a systematic review. Learning Points: LQTS can have normal QTc. mEq/L for K+ and 1.76
Methods Patients were retrospectively evaluated between January 2012 and June 2020. Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chest pain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%).
Free full text: [link] There are 6 categories of criteria : 1) Imaging 2) Pathologic 3) ECG Repolarization 4) ECG Depolarization 5) Arrhythmias 6) Family History. e5 Article Download PDF Google Scholar 3 RNW Hauer, MGPJ Cox, JA Groeneweg Impact of new electrocardiographic criteria in arrhythmogenic cardiomyopathy Front Physiol, 3 (2012), p.
The rhythm is uncertain ( ie, We only see 4 beats — because the same 4 beats are repeated in limb and chest leads — but in lead II there appears to be sinus bradycardia and arrhythmia plus a P wave with a PR interval too short to conduct preceding beat #1 — therefore need for a longer period of monitoring ).
Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. In light of the risk of arrhythmia events observed in the Mizusawa trial, a formal EP study might be reasonable to obtain in those with fever induced asymptomatic Brugada ECG changes to help risk stratify these patients.
Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. In light of the risk of arrhythmia events observed in the Mizusawa trial, a formal EP study might be reasonable to obtain in those with fever induced asymptomatic Brugada ECG changes to help risk stratify these patients.
Electrocardiol 45:433-442, 2012 ). Finally — a detailed family history ( for early sudden death ) + a careful personal history ( for syncope/presyncope; malignant arrhythmia ) is in order. Figure-2: TOP: ECG Brugada-1 and Brugada-2 patterns ( from Bayés de Luna et al: J.
J Electrocardiology 45 (2012):433-442. Conclusion of this paper: Fever is a great risk factor for arrhythmia events in Brugada Syndrome patients. Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. Bayes de Luna, A et al.
2012 Apr 4;4(6):483.) We don’t need to think deep, to realize, modalities which take on this arrhythmia head-on has a minuscule role at the population level. 2012 Oct 6;5(3):647. Al Chekakie MO, Akar JG. Epicardial Fat and Atrial Fibrillation: A Review. J Atr Fibrillation. Circ Arrhythm Electrophysiol. 2010 Jun;3(3):230-6.
While traditionally described as “benign early repolarization”, they have been associated with J wave syndromes along with Brugada syndrome, causing ventricular arrhythmias (1, 2). Europace 2012 Shinde R, Shinde S, Makhale C, Grant P, Sathe S, Durairaj M, Lokhandwala Y, Di Diego J, Antzelevitch C. J wave syndromes.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content