This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. ABSTRACT Introduction The distribution of the origin of focal atrial tachycardia (FAT) in patients with different ages have not been clearly elucidated.
C ASE C onclusion : I lack detailed follow-up from today's case — other than knowing that the Atrial Tachycardia was controlled. This type of Wenckebach response that may be seen with atrial tachycardia ( or atrial flutter ) — is often physiologic, as a result of the rapid atrial rate that occurs with these arrhythmias.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
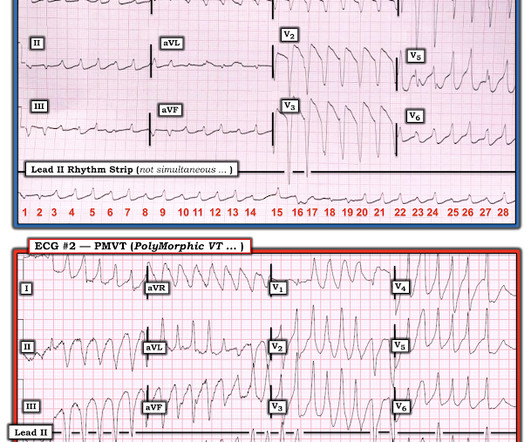
CLINICALLY — the important “take-home” point from this case, is that the shifting QRS morphology despite the constant ventricular rate we saw in ECG #1 — suggests the diagnosis of a pleomorphic VT.
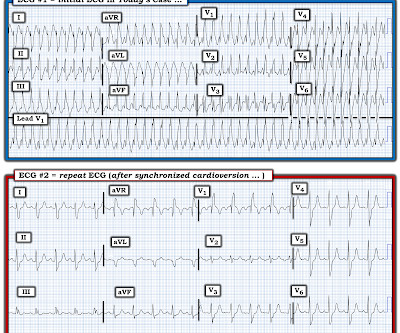
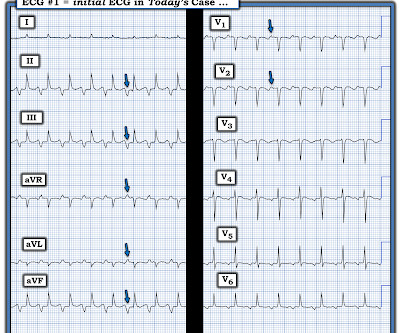
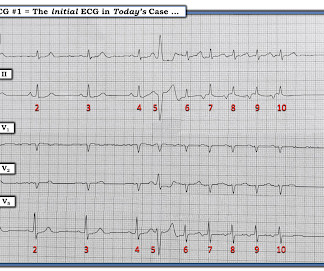
IF today’s rhythm was an SVT — a rate of 250-260/minute is clearly too fast to be sinus tachycardia. Case CONCLUSION: The repeat ECG in Figure-3 shows conversion of the rhythm in ECG #1 to sinus tachycardia ( restoration of upright sinus P waves in lead II — at a rate of ~110/minute ).
You are shown the ECG in Figure-1 — told only that the patient had a “continuous" tachycardia. PEARL # 4: This less common form of "fast-slow" AVNRT that is illustrated in Figure-3 — has also been known as an "incessant" tachycardia. ECG Blog #138 — AFlutter vs Atrial Tachycardia. What is the differential diagnosis?
By this definition, a variety of rhythms may qualify as “SVTs” — including sinus tachycardia, atrial flutter or fibrillation, MAT, AVRT/AVNRT, among others. Why Isn’t this a Run of Atrial Tachycardia? — ECG Blog #138 — AFlutter vs Atrial Tachycardia. ECG Blog #229 — Why AFlutter is commonly overlooked?
Retrospectively — I interpret this 1:1 retrograde conduction as diagnostic of a reentry SVT rhythm as the etiology of the initial tachycardia. As noted by Moodie in his manuscript on Adult Congenital Heart Disease ( Tex Heart Inst J: 38(6):705, 2011 ) — there are now more people over the age of 20 with CHD than under that age!
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
Heart 2011; 97 : 838-843 [link] 14. Hypotension may of course be a result of a brady- or tachydysrhythmia. 2) Hypoxia, including poisons of oxidative phosphorylation such as HS, CO, CN. 3) Anemia, or poisons of hemoglobin such as methemoglobin or CO 4) Fixed coronary stenosis that limits flow. J Am Coll Cardiol. 1985;5(3):711-716.
IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. Multifocal vs Polymorphic VT — September 23, 2011 post from Dr. S.
Methods In a cohort of ATTRwt-CA patients from 2011 to 2022 without prior sustained VA, we ascertained the presence and characteristics of NSVT during clinically indicated ambulatory Holter monitoring. Patients were stratified based on the presence of NSVT at baseline.
Introduction:Supraventricular tachycardia (SVT) is known to affect children and teenagers predominantly but can also occur in adults. in 2011 (APC -5.11 [95% CI -6.08 Circulation, Volume 150, Issue Suppl_1 , Page A4141933-A4141933, November 12, 2024. in adults (above 25 years) from 1999 to 2020. SVT-related deaths were reported.
Here is his 12-lead ECG: The computer reads supraventricular tachycardia. In these cases, they were misdiagnosed as sinus tachycardia (not PSVT): Notice there is a "P-wave" just before the QRS in V1 Notice there is a "P-wave" directly superimposed (on top of) the T-wave in V1. Narrow complex tachycardia at rate of 135.
Chagas disease (ChD) was associated with increased rates of ventricular tachycardia and ventricular fibrillation in ICD patients only in the initial two periods, but there was no statistical difference in the last period. Time periods were chosen based on the establishment of the Arrhythmia Service in 2011.
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). The patient improved, and on Day-11 of the hospital stay — he was off inotropes and on a small dose of a ß-blocker. He required multiple defibrillations within a period of a few hours.
Answer : you must treat the patient's underlying condition causing sinus tachycardia, and repeat the ECG at the lower heart rate. Optimal QT interval correction formula in sinus tachycardia for identifying cardiovacular and mortality risk: Findings from the Penn Atrial Fibrillation Free study. which is 0.6 So is it really prolonged?
There was never ventricular fibrillation (VF) or ventricular tachycardia (VT), no shockable rhythm. Here is a similar case: Collapse, Ventricular Tachycardia, Cardioverted, Comatose on Arrival. Agitation, Confusion, and Unusual Wide Complex Tachycardia. There is sinus tachycardia at ~115/minute.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). This patient very likely has some form of idiopathic ventricular tachycardia. Of the ventricular outflow tract tachycardias (RVOT-VT) makes up 80-90%.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content