This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible. Murakami MM.
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology. Heart 2011; 97 : 838-843 [link] 14.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
In 2011 — Niu et al described the presence of an "N-Wave" — or delayed activation wave of the left ventricular basal region. Because this area of the heart is typically supplied by the LCx — this is likely to be the "culprit" artery when N waves are seen as part of the pattern of acute ischemia ( Int J Cardiol 162(2): 107-111, 2013 ).
But when the clinical presentation is sepsis, one must entertain the possibility that the ST elevation is due to demand ischemia, or some other process, and exacerbated by tachycardia. In this abstract from 2011, we found that 4%(4 of 99) type 2 MI and 38% of type 1 MI had ST Elevation.
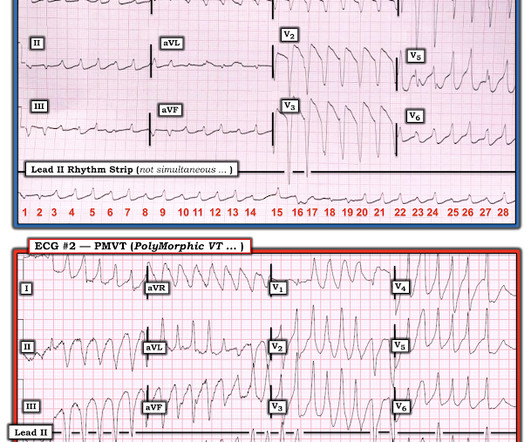
Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. Although IV Mg++ is also indicated as initial treatment of PMVT with a normal QT — it is clearly less likely to respond to IV Mg++, than when the QT interval is prolonged.
At about this point in the process — I like to take a closer LOOK at the 12-lead tracing, to ensure there is no acute ischemia or infarction that might need immediate attention. What about the 1 2- L ead E CG ? As already established — the QRS complex is narrow in all leads, so the rhythm is supraventricular. The QTc is not overly prolonged.
Acute myocardial ischemia. Multifocal vs Polymorphic VT — September 23, 2011 post from Dr. S. As reviewed by Almarzuqi et al ( Vasc Health Risk Mgmt 18:397-406, 2022 ) — Potential Causes of Bidirectional VT include: Digitalis toxicity. CPVT ( Catecholaminergic PolyMorphic VT ). Familial hypokalemic periodic paralysis.
There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( Some residual ischemia in the infarct border might still be present. Both episodes are initiated by an "R-on-T" phenomenon.
When “spot diagnosing” precordial ST-depression I instinctively evaluate aVR for any corresponding ST-elevation to see if an emerging pattern of broad subendocardial ischemia can be appreciated, in which the ST-depression should be otherwise global and demonstrably maximal in Leads II and V5. ST-elevation, etc.) is present. 3] Niu, T.,
In most cases, rather, the culprit is gross ischemia due to myocardial infarction, cardiomyopathy, or advanced coronary artery disease. Unfortunately, today’s case is lacking any such diagnostics, thus I cannot say with certainty that the QT interval is, or is not, culpable in arrhythmogenesis. [1] Elsevier: Philadelphia, PA. [7] 8] Liu, E.,
There is ST elevation in 9/12 leads with ST depression only seen in lead aVR>V1 ( ie, virtually the opposite of what is seen with diffuse subendocardial ischemia in which there is diffuse ST depression except for ST elevation in aVR>V1 ).
That said there were no clinical symptoms or ECG findings suggestive of ongoing ischemia. You have given IV MgSO4 a fast acting -blocker and IV amiodarone bolus and infusion. The possibility of an ischemic cause of the ventricular arrhythmia has to be considered! Troponin T was negative on admission and on repeat blood draw.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content