This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
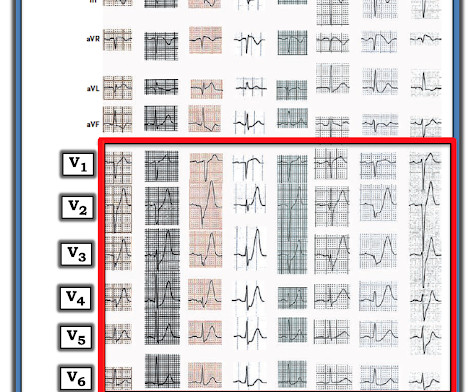
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. The STEMI guidelines do state that hyperacute T-waves "may indicate early acute myocardial infarction" but do not discuss it as a "STEMI equivalent."
This is as clear a STEMI as you can get. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome! This is consistent with MI, though one cannot tell if it is new or old. The structure at the bottom that is moving is the mitral valve, with anterior and posterior leaflets. The Q-wave in lead III persists.
COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. N Engl J Med [Internet] 2019;Available from: [link] Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
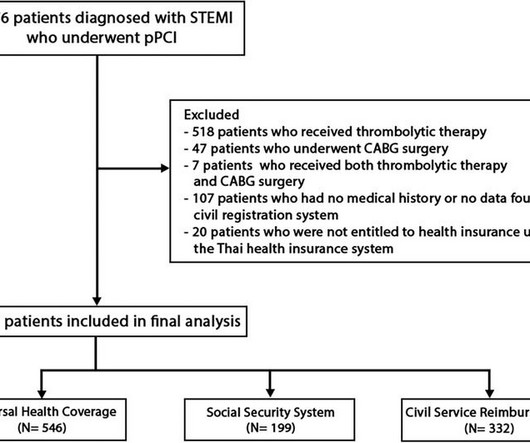
BackgroundIn Thailand, access to specific pharmaceuticals and medical devices for ST-elevation myocardial infarction (STEMI) patients is restricted within certain healthcare systems, leading to inequalities in the quality of medical care among different healthcare systems.
Methods A retrospective clinical cohort study was performed using data from the English National Institute for Health Research Health Informatics Collaborative (2010–2017). to 0.64) after non-ST-elevation (NSTE)-ACS and one-third as likely after STEMI (OR 0.30, 95% CI 0.19 After STEMI, the respective ORs were 1.20 (95% CI 0.84
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. Chicago November 2010.
We found that 38% of out of hospital ventricular fibrillation was due to STEMI. Correlation of STEMI in Resuscitated Non-traumatic out-of-hospital Cardiopulmonary Arrest patients with Initial Rhythm and Cardiac Catheterization Findings (Abstract 580). Academic Emergency Medicine 17(s1):S194; May 2010 Reference : Scott NL.
12:15 — Regarding my experience from the 1980s until ~2010: How I went from hating computer interpretations to loving them ( after I finally understood what the computer can and can not do ). 2:25 — Dr. Grauer: The 1st Error : Too many clinicians in 2024 are still stuck in the outdated millimeter-based STEMI Paradigm”.
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. This difficulty results in high lateral OMI being the most commonly missed OMIs by the misguided STEMI criteria.
At this point — I learned a bit more about today's patient: The patient is a man who had an inferior STEMI in 2010. Evidence of the 2010 inferior infarction ( in the form of large inferior Q waves ) is present in both ECG #1 and ECG #3. We know today's patient had a documented inferior STEMI in 2010.
. = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = ECG Podcast #2 — ECG Errors that Lead to Missing Acute Coronary Occlusion ( Reviewing the concept of OMI — and why the "STEMI Paradigm" is outdated and misses too many acute coronary occlusions! ) — published by Mayo Clinic CV Podcast Series on 1/16/2024 ( 33 minutes ).
Anterior STEMI? A nice Review of EIA by Molis and Molis can be found in Sports Health 2:311-317, 2010. T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. What is it? 2 Cases of Resolved Chest Pain with Dynamic Terminal T-wave Inversion Is it Wellens' Syndrome? Activate the Cath Lab?
This paper by Bischof and Smith compared inferior MI to pericarditis and found that of 154 patients with inferior STEMI, 17% of whom had less than 1 mm of STE in any inferior lead, all 154 had at least 0.25 Maybe an increase in pericardial fluid could have been observed and helped to prevent her acute decompensation one week later.
Using person-linked hospitalisation data, we compared International Classification of Diseases (ICD)-coded data with biomarker-classified admission rates for ST-segment elevation MI (STEMI), non-STEMI (NSTEMI) and unstable angina (UA) in Western Australia (WA).
ECG met STEMI criteria and was labeled STEMI by computer interpretation. J waves can also be induced by Occlusion MI (5), STEMI mimics including takotsubo and myocarditis complicated by ventricular arrhythmias (6, 7), and subarachnoid hemorrhage with VF (8). Take home : Not all STEs are STEMIs or OMIs. What do you think?
BackgroundAcute myocardial infarction (AMI), particularly ST-segment elevation myocardial infarction (STEMI), significantly impacts global health, exacerbated by risk factors such as diabetes mellitus (DM). This study highlights the importance of comprehensive FBG monitoring and management to improve outcomes for STEMI patients.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content