This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundDespite the wellknown importance of witnessed arrest and bystander cardiopulmonary resuscitation (CPR) for outofhospital cardiacarrestoutcomes, previous studies have shown significant statistical inconsistencies. The outcome measure was prehospital return of spontaneous circulation (ROSC).
However, few national population‐based studies have investigated the comprehensive effectiveness of those updates for out‐of‐hospital cardiacarrest due to shockable rhythms. in 2006, and 3.01 in 2015). in 2006, and 3.01
Further research and attention to this area are crucial for improving patient outcomes and guiding clinical interventions in this challenging condition.MethodsICD‐10‐CM codes were used to query the National Inpatient Sample (NIS) for patients with AIS between 2010 and 2019. Patients with AKI were on average older (63.29
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. A reliable study would keep track of all patients with shockable arrest and analyze the ones who were not enrolled to see their outcomes. This is FAR LESS than all other studies of shockable arrest. 5% vs. 58%!!
What is the utility of a head CT in cardiacarrest? We studied this and published the abstract below in 2010. We found intracranial hemorrhage in 2% of non-traumatic cardiacarrest patients, and in 4 others the presence of cerebral edema changed management. Chicago November 2010. Kurkciyan et al.
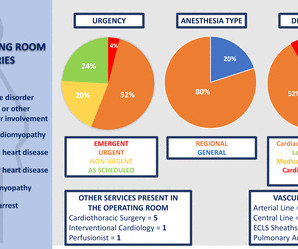
Management of this complex population is not well studied, and little guidance is available regarding labour and delivery planning for optimal outcomes. Study design We performed a retrospective evaluation of pregnant patients with high-risk CVD who delivered in the main OR at a large academic centre between January 2010 and March 2021.
However, none of the formulas have proven to be definitively better than another and none are well correlated with outcomes or events! None is considered definitive due to the paucity of data (and conflicting data) relating QTc to outcomes. JACC 55(9):934-947; 2010 ]. Some other points: 1. This study by Patel et al.
BackgroundDespite the increasing long‐term survival after out‐of‐hospital cardiacarrest (OHCA), the risk of subsequent acute myocardial infarction (AMI) remains poorly understood. Journal of the American Heart Association, Ahead of Print.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content