This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
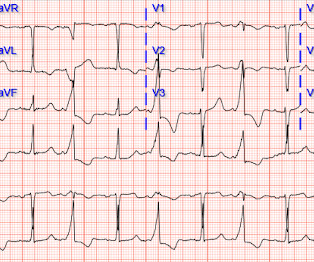
While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. Additionally, the qR morphology, particularly in a patient with right bundle branch block (RBBB) type wide QRS complex tachycardia (WQCT), lends further support for VT. What is the rhythm?
In that study commonest ECG abnormalites were QTc prolongation followed by brady/tachycardia and then ST segment deviations [3]. 2009 Nov;40(11):3478-84. Epub 2009 Aug 27. But the number of persons with lobar hemorrhage in that study was only 17%. doi: 10.1161/STROKEAHA.109.556753. 109.556753.
Notice there is tachycardia. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS. Blackwell Publishing 2009. BP was 160/100. younger smoker).
Another way that WPW can be concealed is in the very rare (~15% of all WPW patients) retrograde-only conduction, in which the accessory pathway ONLY allows retrograde conduction, which obviously wouldn't show a delta wave on sinus EKG but still predisposes the patient to re-entry tachycardias. Epub 2009 Sep 29. References: 1.
Original publication date July, 2009. If this was a tachycardia at a rate of 150, it might appear to be a narrow complex tachycardia, when in fact, it would be a wide complex tachycardia! Concept Review How do you identify right bundle branch block (RBBB) on the 12 lead ECG? In other words, are the QRS complexes “wide”?
NEJM 362(9):779; March 4, 2009. NEJM 362(9):779; March 4, 2009. Hypotension may of course be a result of a brady- or tachydysrhythmia. 2) Hypoxia, including poisons of oxidative phosphorylation such as HS, CO, CN. 3) Anemia, or poisons of hemoglobin such as methemoglobin or CO 4) Fixed coronary stenosis that limits flow. link] 13.
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. J Electrocardiol, 42 (2009), pp. What is the Diagnosis?
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Yield of Diagnostic Tests in Evaluating Syncopal Episodes in Older Patients Arch Intern Med 2009 Jul 27; 169:1299-1305. Sivilotti, M.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content