This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria. In Figure-1 is the ECG from the August 26, 2009 post in Dr. .:
Background Different ST-segment elevation myocardial infarction (STEMI) localizations go along with dissimilarities in the size of the affected myocardium, the causing coronary vessel occlusion, and the right ventricular participation. Results Of the 2,195 patients, 1,118 had an anterior (AWS)- and 1,077 a non-anterior-wall-STEMI (NAWS).
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis. years old ± 13.7
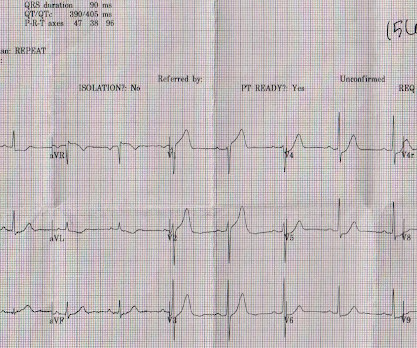
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. Apr 28, 2009.
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0 STE in V4R is confirmatory evidence.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Apr 28, 2009.
” R outine nasal Oxygen has little use in the management of STEMI. tried this in 2009 itself.(Ref 2009 Oct;2(5):366-75. It is tough to consider oxygen as a “powerful and magical drug”, because it is freely available everywhere.” In fact, it can be harmful as it causes vasoconstriction. Stone et al.
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. 2009;Available from: [link] 4.
Background Despite improvements in outcomes of ST elevation myocardial infarction (STEMI), ventricular septal rupture (VSR) remains a known complication, carrying high mortality. The contemporary incidence, mortality, and management of post-STEMI VSR remains unclear. In-hospital mortality was 73.6 ± 1.8%, but only 29.2 ± 1.9
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. Blackwell Publishing 2009.
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. Kurkciyan et al. Chicago November 2010.
As per Dr. Aslanger — a number of medical providers were initial confused by what initially appears as marked ST elevation with reciprocal ST depression, indicative of an acute STEMI. That was also my initial concern. No "baseline" ECG is available for comparison.
Original publication date July, 2009. Generally speaking, right bundle branch block does not mimic, or obscure, the ECG diagnosis of acute STEMI the way left bundle branch block does. This 12-lead ECG shows acute anterior STEMI in the presence of right bundle branch block, but you really need a trained eye to see it.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. NEJM 362(9):779; March 4, 2009. NEJM 362(9):779; March 4, 2009. Look at the aortic outflow tract.
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. Attached is the first ECG.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Inferior infarct, age undetermined.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content