This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology. NEJM 362(9):779; March 4, 2009.
Mechanism is thought to be due to sustained sympathetic stimulation, probably caused by dysfunction of insular cortex resulting in reversible neurogenic damage to the myocardium which could include contraction bands and subendocardial ischemia [2]. 2009 Nov;40(11):3478-84. Epub 2009 Aug 27. doi: 10.1161/STROKEAHA.109.556753.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. Whether it is subendocardial ischemia or posterior STEMI, if you cannot get it to resolve, you must activate the cath lab. There is no ST elevation.
Learning Point: Concordant ST segment elevation can arise from profound ischemia triggered by ventricular tachycardia (VT), or it may represent an exaggerated basal ST change accompanying tachycardia. The patient rapidly regained consciousness, reporting no residual pain. A peak troponin level of 70 ng/L was observed.
Results:Figure 2 shows timecourse of GLC, ATP, and Sodium in different compartments of the model through time in regions experiencing mild and severe ischemia. 2009 Dec 1;27(3):391 A physiologically accurate in silico model would provide a new route for study of the response to an ischemic event. T Ventimiglia et al. 2023;39:e37353.
Chest Pain Severity Rating Is a Poor Predictive Tool in the Diagnosis of ST-Segment Elevation Myocardial Infarction [link] Abstract Current ST-segment elevation myocardial infarction (STEMI) guidelines require persistent electrocardiogram ST-segment elevation, cardiac enzyme changes, and symptoms of myocardial ischemia.
Reference : Apart from the heavily quoted classics of COURAGE, BARI-2D, ISCHEMIA, ORBITA 1 etc. Regular exercise equivalent to PCI (ESC 2009).Will Please note ORBITA -2 is not an antidote to ORBITA-1) ,Read this 1.AVERT AVERT study :Atorvastatin equals PCI.2.Regular Will try to get the link for this soon.
Though this association may be related to impaired cerebral oxygen delivery, it is unclear whether these changes relate to cerebral ischemia. Patients who had a brain MRI and serial hemoglobin measurements were included.
We explored whether major ABO incompatible platelet transfusions are associated with these ischemic lesions.Methods:Consecutive spontaneous ICH patients enrolled into a single-center, prospective cohort study between 2009 and 2016 were assessed. Major ABO incompatible platelet transfusion was the exposure. 217.94, p = 0.03).Conclusions:Major
indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. There is a strong correlation between FFR and inducible myocardial ischemia. It recalculates SYNTAX score by incorporating ischemia producing lesions determined by FFR. 2009 Jan 15;360(3):213-24. Normal FFR is 1.0 N Engl J Med.
This ECG is diagnostic of diffuse subendocardial ischemia. Methods: Between June 2007 - July 2009 all NT-OHCA patients aged >18, transported to our hospital, an urban, level one trauma teaching hospital were included. Chicago November 2010.
Diagnosis of left ventricular hypertrophy in the presence of left anterior fascicular block: A reexamination of the 2009 AHA/ACC/HRS guidelines. Grauer's great explanations on -- LAFB [link] RBBB-LBBB-IVCD [link] LBBB-Sgarbossa-LVH-MI [link] [1] Ravi, S., Annals of Noninvasive Electrocardiology, 18 (1), 21-28. [2] 2] Surawicz, B.
This study aimed to analyze the clinical variables associated with the neuropsychological function in a large cohort of aSAH survivors.Methods:Patients with aSAH admitted to our institution since 2009 were recruited. and in patients who developed new radiological ischemia during hospitalization (OR: 3.42, p 0.03).
Evidence of acute ischemia (may be subtle) vii. in 2010 EM Clinics of North America (full text link) For an Exhaustive Review of Syncope and its full management outside the ED environment, go to the 2009 European Society of Cardiology Guidelines (full text pdf). Arch Intern Med 2009 Jul 27; 169:1262. Left BBB vi. LVH or RV d.
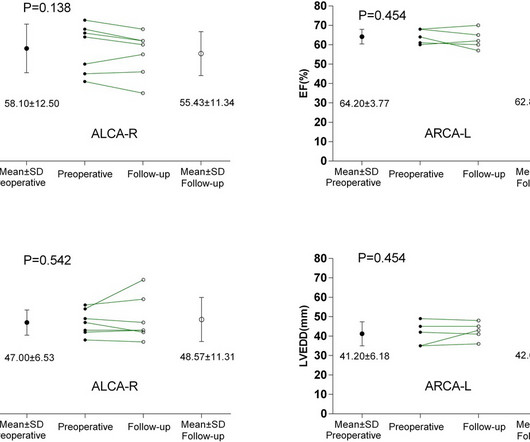
BackgroundAnomalous aortic origin of a coronary artery (AAOCA) is associated with an increased risk of myocardial ischemia and sudden cardiac death. ResultsThe median age at surgery was 26 years (range, 13–57 years). ResultsThe median age at surgery was 26 years (range, 13–57 years).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content