This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
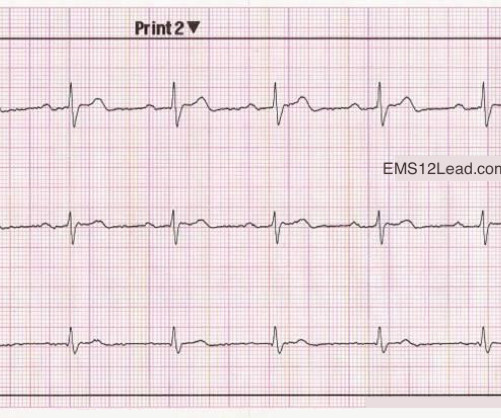
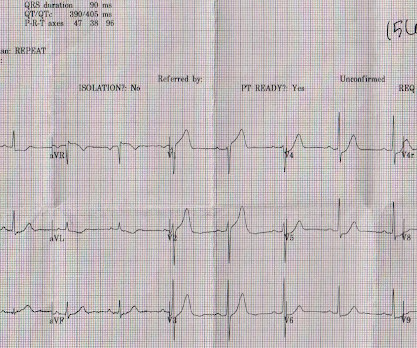
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
Methods We retrospectively analyzed the measurements at rest for 191 patients with acute chestpain (ACP) magnetocardiographically. All included ACP patients were recruited in 2009 at Yonsei University Hospital and were followed up until 2022.
However ,we have some effective clinical and pathological markers too, for effective re-vascularisation They are clinical well being and good functional capacity , relief from chest-pain, reduction of plaque volume, plaque stabilisation, maintenance of collaterals , microvascular patency , reduction of recurrent events.
Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. There is some ST-segment elevation in DII, DIII, aVF, V4-6. Due to the observed ST-segment elevation, the medical team expressed immediate concern.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. Blackwell Publishing 2009.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. Apr 28, 2009. There was some SOB. He had walked into the ED (did not use EMS). Here is his ECG: There is atrial fibrillation at a rate of 95.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. Apr 28, 2009. There was some SOB. He had walked into the ED (did not use EMS). He was in no distress and vital signs were normal. Obviously there is MI.
Original publication date July, 2009. Case Review EMS is called to the residence of a 69 y/o M with a chief complaint of chestpain. Concept Review How do you identify right bundle branch block (RBBB) on the 12 lead ECG? s) Terminal R wave in lead V1 Slurred S wave in lead I Let’s look at an example.
A 36 yo male smoker presented to the ED with chestpain. It had started the night before as "indigestion" and had progressed to 8/10 substernal chest pressure radiating to the right shoulder/jaw associated with diaphoresis, nausea, and SOB. 2009) similarly found that STE in aVR correlated with proximal (vs.
She denied chestpain and denied feeling any palpitations, even during her triage ECG: What do you think? J Electrocardiol, 42 (2009), pp. Her symptoms started suddenly about 48 hours ago, but had continued to worsen, including epigastric discomfort, nausea, cough, and dyspnea and lightheadedness on exertion.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. NEJM 362(9):779; March 4, 2009. NEJM 362(9):779; March 4, 2009. The paramedic’s initial impression of the patient was that he was critically ill.
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. The patient has a history of CABG so some of these changes could be old, but with ongoing chestpain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. Eur Heart J 2009 4 Lemkes et al.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Arch Intern Med 2009 Jul 27; 169:1262. Arch Intern Med 2009 Jul 27; 169:1305.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content